Executive summary
Antimicrobial resistance is one of the most serious global One Health threats of the 21st century, linking the interests, concerns and efforts of human health, animal health, and environmental health. Documented in almost all regions of the world,1 antimicrobial resistance is considered by many as the silent global pandemic that will undermine healthcare systems and food safety and supply, and result in millions of deaths.
The current estimated economic and human costs are large enough to justify major intervention, however this threat continues to go unnoticed by many. Studies suggest that resistant infections can add an additional AUD$10,000 to the cost of treatment,2 and that Australian hospitals spend an additional AUD$16.8 million per year treating common resistant hospital-associated infections.2 Antimicrobial resistance was associated with 4.95 million deaths in 2019,3 and over the next few decades it is predicted to become one of the leading causes of death, estimated to be responsible for 10 million deaths each year by 2050.4,5
While antimicrobial resistance is a natural phenomenon, the largely unrestrained use of antimicrobials in human and animal health and agriculture combined with several other complex factors is accelerating the emergence and spread of resistant pathogens. Of these factors, the failing market for antimicrobial development has meant that the breadth and novelty of the current pipeline of new antimicrobials is insufficient to meet the ongoing threat of antimicrobial resistance. Without new antimicrobials, the world may be on track to return to the medical ‘dark ages’, a time where a superficial scratch could be life threatening, and the procedures and treatments which we now rely on are considered too risky to perform, due to risk of untreatable infection.
Antimicrobial resistance requires a global response, and one country’s actions will not have a significant impact if other nations continue to act independently of one another. As a wealthy, developed country with an advanced healthcare system, Australia is well placed to lead global efforts to control the growing threat of resistant infections and other health threats, particularly in the Asia-Pacific region. Australia however is lagging in several key areas, including public awareness and understanding of antimicrobial resistance; stewardship; coordination and incentives for research and development; and national One Health governance. To address this, the AMA has proposed several solutions that build on work the government is already doing to encourage behavioural change, incentivise antimicrobial research and development, and deliver a unified One Health approach to tackling antimicrobial resistance. These solutions include:
- establishing a Centre for Disease Control (CDC) that is a recognised separate authority for the national scientific leadership and coordination of diseases and health threats, as well as several immediate priorities for government to ensure Australia’s response to antimicrobial resistance is effective, integrated, and aligned to One Health objectives
- improving antimicrobial stewardship practices in Australia, by embedding stewardship practices, education and training, and clinical decision support tools into all sectors
- improving the antimicrobial market through sovereign manufacturing of antimicrobials and implementing mechanisms to incentivise research and development.
The need for efficient, effective, and sustainable mechanisms to prevent and treat infectious diseases was clearly demonstrated during the COVID-19 pandemic. These proposed solutions will position Australia as a global leader and support a coordinated, sustained, and unified One Health approach to addressing antimicrobial resistance and other health threats. Now is the time for strong and sustained action on antimicrobial resistance, as this may well be the cause of the next global pandemic.
The global threat of antimicrobial resistance
Infectious diseases, which are caused by microorganisms such as viruses, bacteria, fungi, or parasites have long been a source of mortality and morbidity, costing the Australian health system $7.5 billion in 2018–19, which is 5.62 per cent of health spending.6 The prevention and treatment of infectious diseases relies on antimicrobials, such as antivirals, antibiotics, antifungals and antiparasitics, which either destroy or inhibit the growth of the microorganisms.
The discovery of antimicrobials was one of the most significant developments for humanity, enabling treatment of many communicable and fatal diseases such as tuberculosis, malaria, and human immunodeficiency virus (HIV). Antimicrobials have also enabled significant advancements in healthcare that would have otherwise been unachievable. For example, many patients are prescribed prophylactic antibiotics to reduce the risk of bacterial infections when undergoing surgery, and early antibiotic therapy can be lifesaving in patients who are receiving immune-suppressing therapy such as chemotherapy for cancer.7,8
Antimicrobial resistancei is a natural phenomenon that occurs when microorganisms change in ways that render antimicrobials less effective. Microorganisms may evolve resistance mechanisms or may acquire it through transfer of genetic material from one microorganism to another. Patients infected with a resistant microorganism are less likely to recover with the first antimicrobial therapy prescribed and are therefore likely to require second- or third-line antimicrobials and treatments, which are more expensive and may have serious side effects. The delay in effective treatment increases morbidity, and some infections do not respond to any available antimicrobials, which often results in severe illness or death. With antimicrobial resistance now documented in almost all regions of the world, it is now considered to be one of the leading global public health threats of the 21st century.1
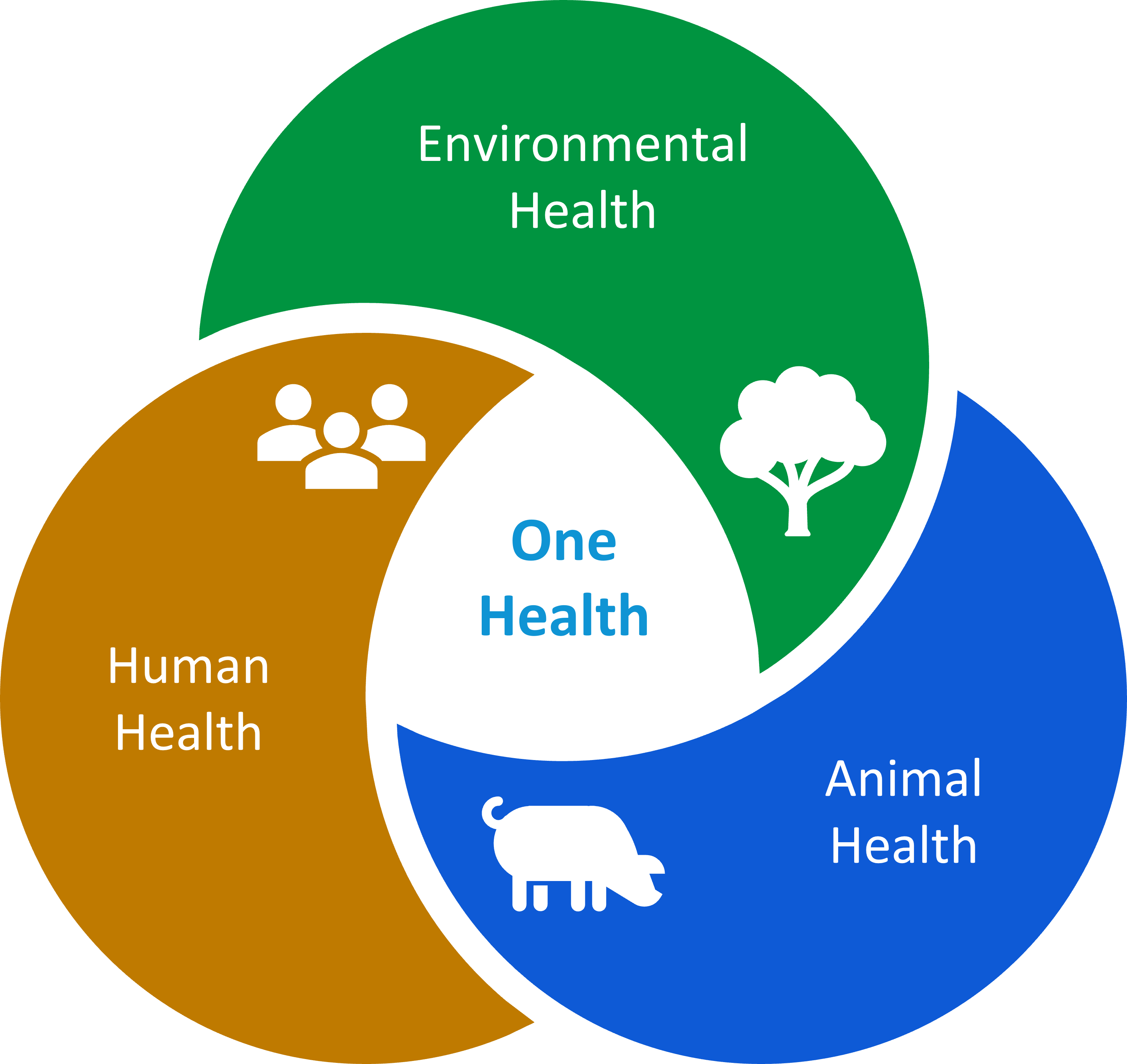
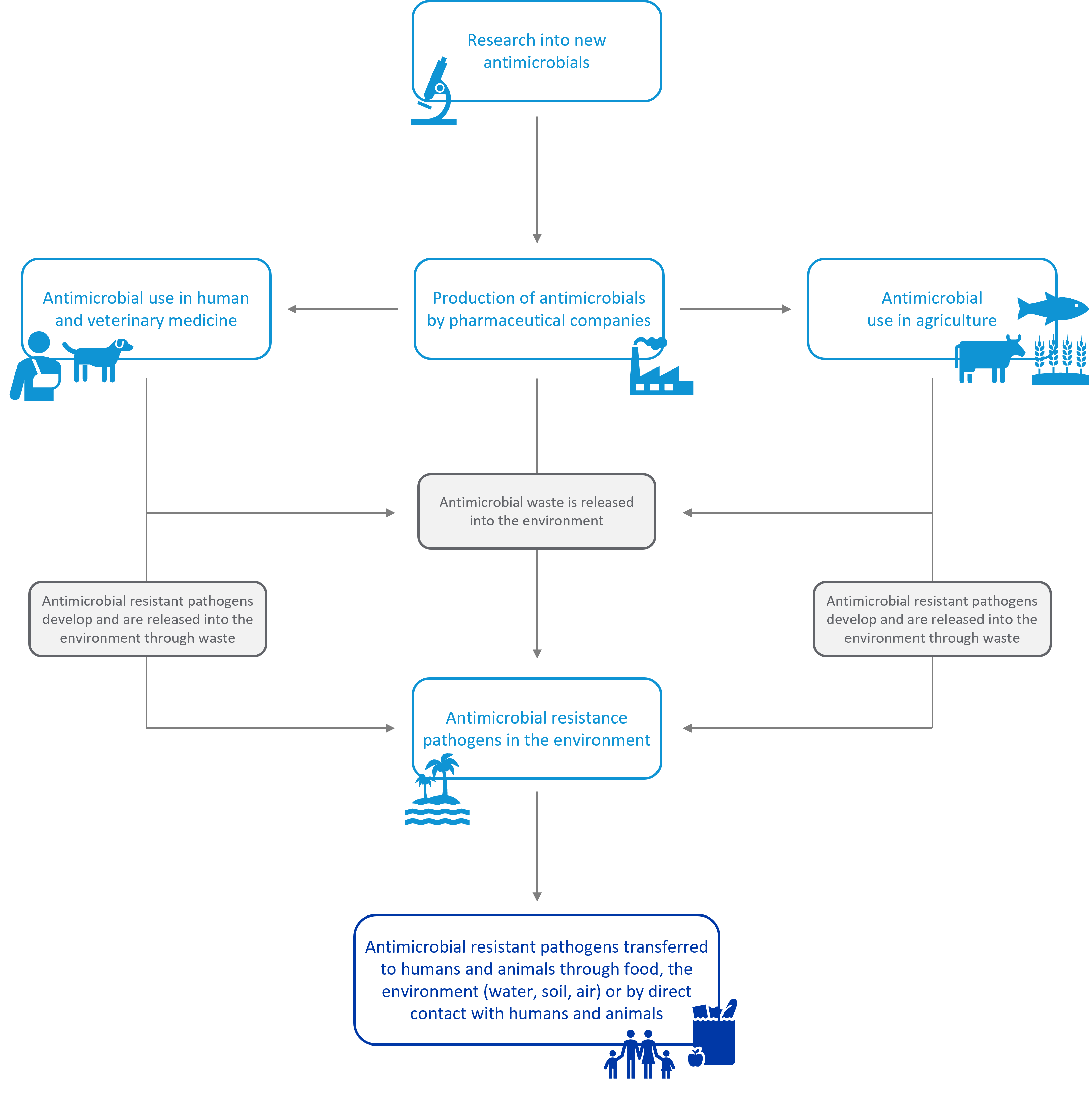
Commonly referred to as a ‘One Health’ issue (Figure 1), antimicrobial resistance links the interests, concerns and efforts of human health, animal health, and environmental health, with the threat interconnected across these sectors (further depicted in Figure 2). Addressing antimicrobial resistance therefore requires an integrated and unified approach.
Factors accelerating the emergence and spread antimicrobial resistance globally
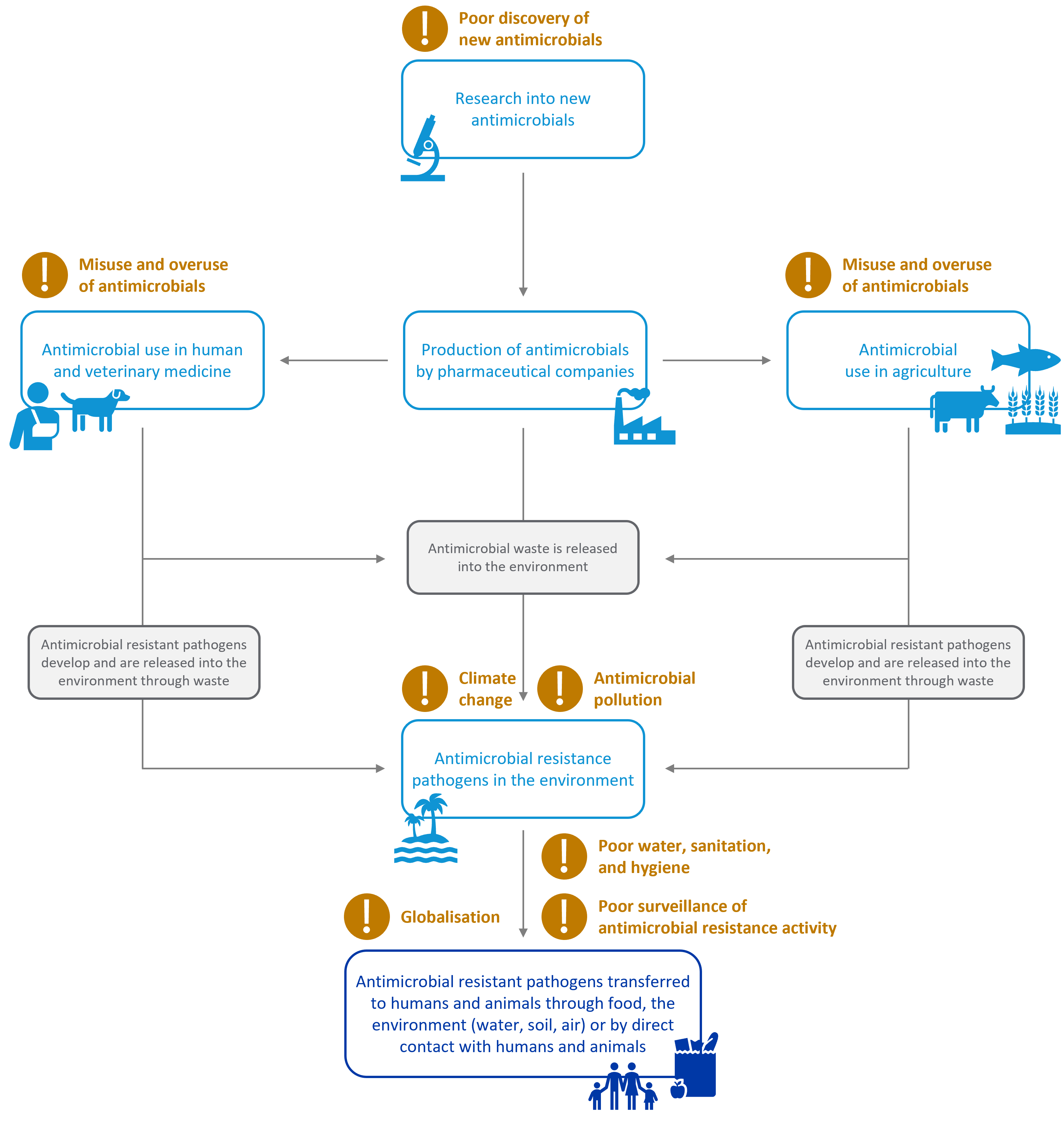
While antimicrobial resistance occurs naturally over time, the largely unrestrained use of antimicrobials in human and animal health and agriculture combined with several other complex factors is accelerating the emergence and spread of resistant pathogens. These factors are summarised in Figure 4.
Misuse and overuse of antimicrobials in human and veterinary medicine
The use of antimicrobials, even when they are used appropriately and conservatively, increases the selection of resistant strains, and contributes to the development of antimicrobial resistance. The misuse and overuse of antimicrobials is therefore a key driver in the development of drug-resistant pathogens, particularly in countries where there is poor regulation and stewardship of prescription of antimicrobials. For example, antibiotics, antivirals and antimalarials can be easily obtained without a prescription in several countries, including India, Thailand, and Nepal.9,10,11,12 With studies suggesting that most people generally have limited knowledge about the correct use of antimicrobials, this availability of over-the-counter antimicrobials results in patients self-medicating and treating diseases with the incorrect medication, particularly the use of antibiotics to incorrectly treat viral diseases such as the common cold or flu.13,14,15 Poor regulation of the manufacturing of antimicrobials in developing countries, particularly antimalarials and antibiotics, is also resulting in the production and distribution of substandard and counterfeit drugs.16 In some countries physicians are even incentivised to prescribe antibiotics as they receive funding from pharmaceutical companies, resulting in high rates of over-prescribing.17
In Australia, rates of antimicrobial prescribing and dispensing have steadily decreased over the last few years due to the implementation of various initiatives aimed at identifying areas of excessive prescribing and improving awareness of antimicrobials resistance. Despite these decreases, a recent report compiled by the Australian Commission on Safety and Quality in Health Care however revealed that prescribing rates, particularly of antibiotics, continue to remain high.18 When compared to similar Organisation for Economic Co-operation and Development (OECD) countries, Australia had 22.7 defined daily doses of antimicrobials medicines dispensed for every 1,000 Australians per day in 2017–18,18 which is more than double the equivalent figure in the Netherlands (8.9) and Sweden (10.8).19 Studies show that this high prescribing rate is likely due to a combination of factors, including:
- delays in diagnostic tests or cultures and the risk of the infection progressing if timely care is not provided
- time constraints in a consultation to undertake a detailed assessment
- patient expectations and pressure
- the absence of antibiotic prescribing guidelines that are integrated with electronic medical records and clinical workflow.20,21
In addition to high rates of prescribing, studies show that many Australians are misusing antimicrobials, including using leftover antibiotics from the last unfinished course the next time they are unwell, sharing unused medications with other people, and disposing of unused or expired antibiotics in household waste (refer to Antimicrobial pollution).22,23
Misuse and overuse of antimicrobials in agriculture
While the misuse and overuse of antimicrobials in human and veterinary medicine needs to be addressed, it is worth acknowledging that the majority (an estimated 73 per cent24 worldwide and 60 per cent25 in Australia) of antimicrobials are consumed by animals as part of farming and animal husbandry. Antimicrobials are also commonly used in other agricultural practices, including crop production and aquaculture.26,27 The use of antimicrobials in agriculture helps to prevent and treat diseases and has become an essential mechanism to improve yields.28,29 Our growing global population however has resulted in excessive use of antimicrobials to promote growth of livestock and counteract the consequences of poor and intensive farming conditions.29 For example, colistin, a critical last-line antibiotic used to treat severe infections in humans, is used in animal farming worldwide to promote growth of livestock.30 This excessive use of antimicrobials in agriculture is a significant contributor to the development of antimicrobial resistance.31
As a major food producer and exporter, Australia has strong regulations on the use of antimicrobials in agriculture and is considered to have a relatively conservative approach. For example, colistin, and several other antimicrobials that are important for human health, are not approved for promoting growth of livestock in Australia.32 Additionally, animal husbandry regulations in Australia are relatively advanced with regular monitoring for antimicrobial resistance.33 These regulatory mechanisms however are considered to be insufficient, with studies finding high proportions of antimicrobial resistant bacteria in Australian beef and salmon.34,35,36
Climate change and increasing global temperature
Climate change and antimicrobial resistance are two of the most imminent global problems and health threats facing humanity. While both climate change and antimicrobial resistance are significant issues in their own right, there is strong evidence to suggest that these two global challenges are interlinked, with increasing global temperatures due to climate change facilitating the release of ancient resistant pathogens, as well as accelerating the emergence of new resistance.
The survival, reproduction, and transmission of pathogens is highly dependent on factors such as temperature, humidity, and precipitation.37 Research indicates that the higher temperatures and extreme weather events associated with climate change are creating environments that increase transmission of infectious diseases and favour the growth and survival of resistant pathogens.37,38,39,40,41 For example, extreme weather events such as storms with high precipitation and floods create conditions that favour the transmission of vector-borne diseases (e.g. malaria, Japanese encephalitis, and dengue fever),42 enteric diseases (e.g. cholera, rotavirus, and giardiasis)43 as well as parasitic diseases (e.g. schistosomiasis).44 Additionally, increases in environmental temperatures are associated with increased resistance, with a recent study demonstrating that an increase in temperature of 10oC resulted in an increase in antibiotic resistance of 4.2 per cent for Escherichia coli, 2.2 per cent Klebsiella pneumoniae, and 3.6 per cent for Staphylococcus aureus.45 A similar study also revealed that higher temperatures are associated with more rapid increases in resistance.46 Climate change is therefore creating conditions that are favouring the proliferation and spread of resistant pathogens.
The increasing global temperature due to climate change is also resulting in rapid thawing of the cryosphere, which is the portion of the Earth where water is permanently frozen, such as glaciers, ice sheets and permafrost.ii As the cryosphere thaws, ancient pathogens that possess naturally resistant genes are being released into the environment. For example, a recent study of the Arctic permafrost region revealed 70 unique antimicrobial resistant genes in microbes against 18 antimicrobial drug classes in this permafrost region.47 Another study found antibiotic resistant genes in samples from various glaciers in Central Asia, North and South America, Greenland, and Africa.48 The permafrost also contains huge stores of greenhouse gases, including methane, carbon dioxide, and nitrous oxide. When the permafrost melts, these gases are released into the atmosphere and trap heat close to the Earth’s surface, therefore contributing to global temperature increases and further fuelling the melting of the cryosphere.49
The healthcare industry in particular is a significant driver of greenhouse gas emissions, a primary driver of climate change. In Australia, the carbon footprint attributed to healthcare is estimated to be 7 per cent of Australia’s total carbon footprint.50 In comparison, carbon emissions attributed to healthcare in the United Kingdom are only 4 per cent of total emissions, despite the spend on healthcare being comparableiii to that of Australia. Although hospitals make up the largest share of carbon emissions in Australia, the footprint of the sector is multi-faceted, including pharmaceutical production, the design of medical infrastructure, procurement, and private medical practice. Additionally, carbon emissions do not represent the total environmental impact of healthcare in Australia, with factors such as waste production and water usage also significant contributors to the impact of healthcare on the environment, particularly during the COVID-19 pandemic with the increased use of personal protective equipment (PPE), water for sanitation, pharmaceutical production, and disinfectants.
The AMA and Doctors for the Environment (DEA), amongst others, are calling for the Australian healthcare sector to reduce its significant emissions, 80 per cent by 2030 and net zero emissions by 2040 (in line with meeting the 1.5oC Paris Agreement target).51,52,53,54 To achieve this goal many organisations, including the AMA, are calling for the establishment of a national sustainable development unit to build on existing efforts and drive environmental sustainability in a coordinated way. Further outlined in the AMA’s position statement Environmental Sustainability in Health Care, the sustainable development unit would coordinate and streamline integrate the efforts of governments, the private sector, and not-for-profit organisations. It would also be responsible for setting clear and accountable targets, developing tools and guidance to support achieving these targets, and measuring progress against these targets by monitoring healthcare carbon emissions along with other indicators of environmental impact.55 Reducing the impact of the healthcare industry on the environment will contribute to the reduction of antimicrobial resistance and improve broader health outcomes for Australians.56
Improved global living standards and increased income in low- and middle-income countries
Globally, there has been an increase in antimicrobial use over the last two decades, which can be in part attributed to the increased use in developing countries as a result of increased incomes and improved living standards.57 For example, the largest consumers of antibiotics in 2000 were the United States, Spain, New Zealand, France and Hong Kong, however in 2015 several low- and middle-income countries including Turkey, Tunisia, Algeria and Romania were considered some of the largest consumers.58 As living standards and incomes continue to rise in low- and middle-income countries, it is anticipated that use and overuse of antimicrobials will continue.
Global connectedness
The COVID-19 pandemic revealed how challenging it is to contain and prevent transmission of emerging and re-emerging infectious diseases in the current era of global connectedness. For example, research suggests that around 30 per cent of international travellers acquire antimicrobial resistant bacteria during travel,59 including travellers returning to Australia.60,61 Additionally, growth in medical tourism[1]has accelerated the international spread of healthcare acquired infections,62,63 particularly as many popular destinations for medical tourismiv, such as Thailand, India, and Malaysia, are also countries with high rates of antimicrobial resistance.64,65,66,67 As the international movement of people, animals, foods, and other products continues to increase, so will the emergence and spread of resistant pathogens.
Poor surveillance of antimicrobial resistance and use
Integrated surveillance of antimicrobial resistance and antimicrobial use across One Health sectors is critical for effective and evidence-based policy, stewardship, and control of antimicrobial resistance. While global surveillance of antimicrobial use and resistance is one of the key priorities of the World Health Organization (WHO) and is being actioned through their Global Antimicrobial Resistance and Use Surveillance System, many countries do not systematically gather data on the use of antimicrobials or conduct regular surveillance to determine the prevalence of resistant pathogens.68 Additionally, the COVID-19 pandemic has placed enormous pressure on healthcare systems and diverted resources, personnel, and attention away from the surveillance of antimicrobial resistance.69 This poor surveillance of antimicrobial resistance and use ultimately makes it challenging to ascertain the scale of antimicrobial resistance globally, coordinate efforts to address antimicrobial resistance, and determine the efficiency of these efforts.
Failing market for the development of novel antimicrobials
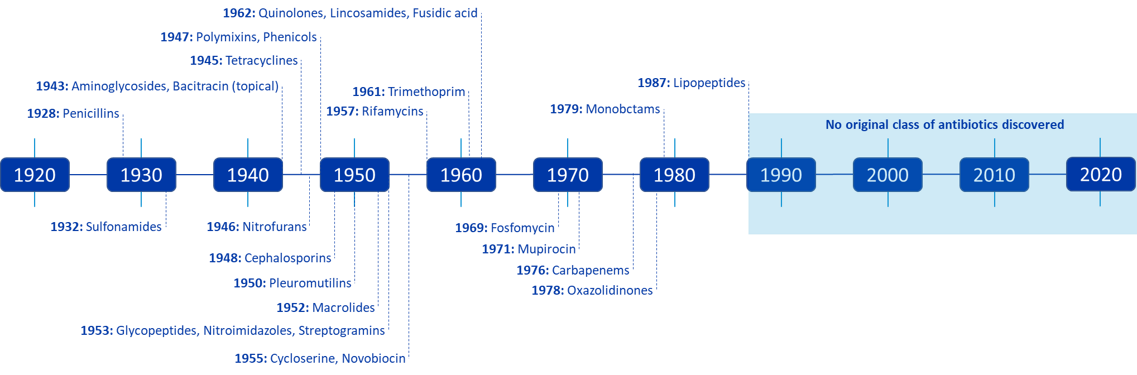
The discovery of antimicrobials, in particular antibiotics, has been one of the greatest contributions to medical advancement. While there was a steady discovery of new classes of antibiotics between 1928 and 1987, there has been no original class of antibiotic discovered for more than three decades (Figure 3), with all antibiotics brought to market being variations of those that have been discovered before. The current development pipeline is therefore insufficient to meet the ongoing threat of antimicrobial resistance.
Despite the huge societal costs of antimicrobial resistance and urgent need for novel antimicrobials and antibiotics in particular, the market for manufacturing these drugs is largely unviable for a variety of reasons, including:
- nearly all new antibacterial treatments are categorised as “reserve” antibiotics for where there are no other alternative treatments, limiting their sales volume and making it challenging to generate income and therefore profits
- resistance development can be fast, resulting in low profits for a company as new antimicrobials may only be viable for a short time
- pharmaceutical companies find the regulatory requirements unclear, which has led to uncertainty about drug approval
- antimicrobials are technically difficult to develop and there is a high failure rate, as they need to reach the target area of the body at a high enough concentration, without being toxic, and then neutralise the microbe
- there are few incentives and government funding to support research and development
- a relatively small number of patients contract antimicrobial resistant infections and meet the requirements to participate in clinical trials.70,71,72,73,74
This is known as ‘market failure’, as the market requires intervention to limit the use of antimicrobials to prevent resistance, which makes it challenging for pharmaceutical companies to receive a return on investment.
For example, a study from 2017 estimated that the cost of developing an antibiotic is around US$1.5 billion, with the average revenue generated from an antibiotic’s sale estimated to be around $46 million.74,75 This market failure has resulted in many large pharmaceutical companies dropping out of the market in favour of more profitable drug development, such as cancer treatments.74 The preclinical and clinical pipeline is therefore driven by small- and medium-sized pharmaceutical companies, researchers, and funding bodies, which struggle to obtain funding for late-stage clinical development up to regulatory approval. Currently there are only 64 unique new antibacterial therapeutics in the clinical pipeline, which is considered to be insufficient to meet the ongoing threat of wide-spread infection from resistant pathogens.76 When compared to other diseases such as cancer, where there are 160 unique therapies in the clinical pipeline for breast cancer alone, it is evident that the market for developing antibacterial therapeutics is failing.76 This issue has been raised by many sector stakeholders, including the Pharmaceutical Benefits Advisory Committee who statedv that the Pharmaceutical Benefits Scheme (PBS) does not easily accommodate new antibiotics intended for use against resistant microorganisms, as new pharmaceuticals are evaluated on their value for money as opposed to the value they may bring to society.77
Antimicrobial pollution
Antimicrobials can pollute the environment through human and animal waste, improper disposal and handling of unused drugs, medical waste, direct environmental contamination from agriculture and aquaculture, or via pharmaceutical waste from the production of antimicrobials.78,79 For example, several studies have identified antibiotic resistant bacteria in wastewater samples for common bacteria such as Escherichia coli,80 as well as concerning antimicrobial resistant genes such as the colistin resistance gene mcr-1.81 High levels of antimicrobial resistance have also been identified in pharmaceutical wastewater, particularly in countries such as India where regulations for the release of pharmaceutical waste are minimal.82 A report by the investigative agency Ecostorm found that 16 of 34 pharmaceutical manufacturing sites in India were found to be harbouring bacteria resistant to antibiotics.83
Antimicrobial pollution has received comparatively less focus than other drivers of antimicrobial resistance. There is however strong evidence to suggest the release of antimicrobial compounds in the environment where there is a diverse antimicrobial ecosystem in soil and water is driving bacterial evolution and the emergence of antimicrobial resistance.78,79,84,85 While microbes in water and soil naturally possess a huge diversity of resistance genes, the sublethal doses of antimicrobials in the environment generates selective pressure on microbes to acquire resistant genes. These antimicrobial resistant pathogens can then be transmitted back to humans and animals through drinking water, food consumption or through direct contact with the environment.86,87,88,89,90
Early studies indicate that the COVID-19 pandemic has substantially contributed to antimicrobial pollution due to the increased use of biocides, antibiotics, antivirals, and disinfectants, which has resulted in the unintended release of these antimicrobials into wastewater and sewage treatment plants.91 At the same time, human and financial resources have been diverted away from antimicrobial stewardship efforts and other mechanisms to reduce antimicrobial pollution. 92,93,94,95 It is therefore likely that the COVID-19 pandemic has, and will continue to, accelerate the selective survival of resistant pathogens in the environment.
Poor water, sanitation, and hygiene
Research indicates that poor water, sanitation, and inadequate infection prevention through hygiene is associated with antimicrobial resistance, as it promotes the spread of resistant microbes, as well as increases the need for antibiotic use to treat infections.96 Studies show that unhygienic conditions are a major cause of antimicrobials use in low- and middle-income countries, and that improvements in water and sanitation infrastructure have played a fundamental role in reducing the burden of infectious diseases and the need for antimicrobials globally.97,98,99 Many people in low- and middle-income countries, however, continue to live in poverty without access to these basic services, with approximately one in three people worldwide living without access to improved sanitation. This may be one of the reasons why the burden of antimicrobial resistance is disproportionally higher in low-income and middle-income countries.5
The case for change: The health and economic burden of antimicrobial resistance
Antimicrobial resistance has now been documented in almost all regions of the world,1 and is considered by many as the silent global pandemic that will undermine healthcare systems and result in millions of deaths. Our poor understanding of antimicrobial resistance activity in human health, animal health, food, agriculture, and the environment is one of the biggest barriers to understanding the true burden of resistance globally, as well as in Australia. In recent years however, several studies have endeavoured to estimate the national and global burden on patients, the health care system, and the broader economy.
Burden of antimicrobial resistance on patients
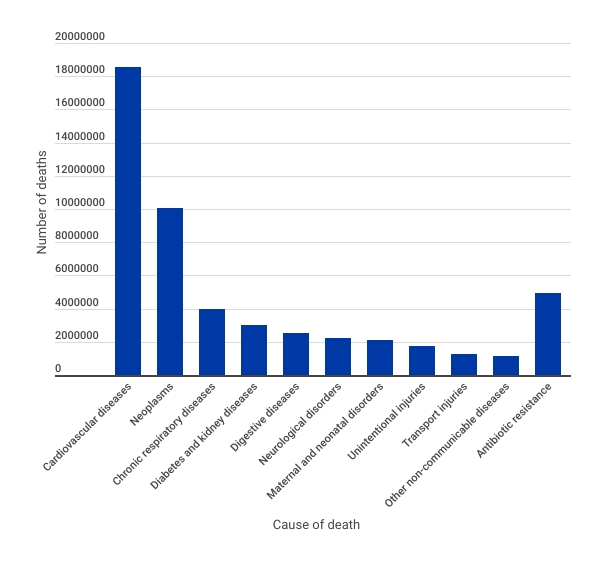
A large and comprehensive study was recently undertaken to assess the burden of antibiotic resistance based on estimates for 204 countries and territories. Using the 2019 Global Burden of Diseases, Injuries, and Risk Factors Study (GBD), it was estimated that 4.95 million deaths in 2019 were associated with antibiotic resistance, with 1.27 million of those deaths directly attributable to a resistant bacterial infection.3 Of these deaths, lower respiratory and thorax infections, bloodstream infections, and intra-abdominal infections accounted for 78.8 per cent of deaths attributed to antibiotic resistance.3
Depicted in Figure 5, it is evident that antibiotic resistance presents a major threat to human health when compared to the top 10 causes of death resulting from non-communicable diseases, disorders and injuries. With studies suggesting that antimicrobial resistance could be responsible for 10 million deaths each year by 2050, it may become one of the leading causes of death over the next few decades.4,5 Additionally, patients who acquire antimicrobial resistant infections have worse outcomes, requiring second- or third-line antimicrobials and treatments which often have significant side effects, including nerve damage, organ failure, and hearing loss.100,101,102,103 Like many diseases, the health risks associated with antimicrobial resistance disproportionately affect the vulnerable and disadvantaged, including older populations, ethnic communities, those who are immunocompromised or have other underlying comorbidities, lower socioeconomic communities, children, and those who live in remote areas.104
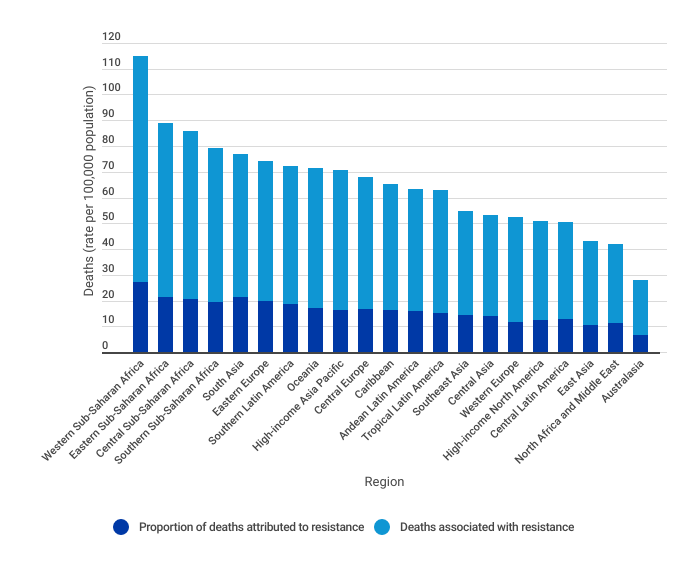
Of the 204 countries and territories analysed (which were aggregated into 21 regions), the Global Burden of Disease Study 2019 study found that Australasia had the lowest rates of deaths per 100,000 population associated and attributed to antibiotic resistant bacteria in 2019, compared to the other regions in the analysis (Figure 6). Growing rates of antimicrobial resistance globally and increasing global connectedness, combined with the insufficient pipeline of antimicrobial discovery, presents a significant health risk to Australia, particularly as resistant pathogens, like all pathogens, do not respect geographic borders.
While this comprehensive study focused on antibiotic resistant bacterial infections, antimicrobial resistance presents a serious threat for global fights against many non-bacterial infectious diseases. For example, the number of HIV presentations that are resistant to antiretroviral therapy is on the rise, with the WHO reporting that more than 10 per cent of adults and 50 per cent of infants commencing treatment for HIV treatment having resistance to first line antiretroviral therapies.106 There have also been increased reports of resistance to antimalarials, particularly in Africa where 90 per cent of malaria cases are reported.107,108
Burden of antimicrobial resistance on socioeconomically disadvantaged populations
Studies show that socioeconomically disadvantaged populations are disproportionally impacted by antimicrobial resistance, in particular methicillin-resistance Staphylococcus aureus (MRSA), due to a variety of reasons including crowded housing conditions, poor access to healthcare, poor hygiene, higher rates of infection, and higher rates of antimicrobial use.109 Aboriginal and Torres Strait Islander peoples in particular are more likely to suffer from infections requiring antimicrobial treatment and antimicrobial resistance, with one study indicating that Aboriginal and Torres Strait Islander peoples are 5.9 times more likely to have a Staphylococcus aureus infection, and 29.2 times more likely to have a community-associated MRSA infection compared to non-Indigenous Australians.109
Burden of antimicrobial resistance on healthcare system
Antimicrobial resistance presents a large burden to the financial sustainability of the healthcare system as well as to broader economic productivity. While the cost to the healthcare system largely depends on factors such as the type of resistant pathogen, where the patient is receiving care, and the comorbidities of the patient, studies suggest that the additional healthcare costs associated with antimicrobial resistance can be more than double the cost of treating an antimicrobial susceptible infection.110,111,112,113 This is due to a variety of factors, including the need for more aggressive second-line and third-line therapies which are often more expensive, the development of complications, the need for more expensive diagnostic tests and procedures, and longer hospital stays. A recent study of Australian hospitals revealed that a resistant infection can add an additional AUD$10,000 to the cost of treatment when compared to a susceptible infection.2 It also revealed that Australian hospitals spend an additional AUD$16.8 million per year treating the five most clinically relevant resistant hospital-associated infections.2 While this may seem insignificant now, this cost will only continue to increase as the global burden of antimicrobial resistance increases. Additionally, these costs are not representative of the broader economic burden of productivity loss, personal costs, and the costs of premature death. It is estimated that by 2050 the annual impact of antimicrobial resistance on the Australian economy will be between $142 billion and $283 billion (under a worst-case scenario), and between $80 and $90 trillion worldwide.114,115,116
The promises and pitfalls in Australia’s antimicrobial resistance response
As antimicrobial resistance has increased and emerged as a global health risk, so too have the calls for national and international efforts to slow its development. The WHO has taken the lead in driving global efforts, and in May 2014 the World Health Assembly, the decision-making body of the WHO, adopted a resolution to develop a global action plan on antimicrobial resistance. The Global Action Plan on Antimicrobial Resistance outlines five strategic objectives to tackle antimicrobial resistance:117
| 1 | Improve awareness and understanding of antimicrobial resistance through effective communication, education, and training |
| 2 | Strengthen the knowledge and evidence base through surveillance and research |
| 3 | Reduce the incidence of infection through effective sanitation, hygiene, and infection prevention measures |
| 4 | Optimise the use of antimicrobial medicines in human and animal health |
| 5 | Develop the economic case for sustainable investment that takes account of the needs of all countries, and increase investment in new medicines, diagnostic tools, vaccines, and other interventions |
This global action plan outlines the need for a One Health approach whereby actions are coordinated across all sectors to recognise the interdependency between people, animals, plants, and the shared environment and ecosystems. In the context of antimicrobial resistance, this would require collaboration across all sectors where antimicrobials are used at a local, regional, national, and global level to ensure efforts are aligned and holistic.
The global action plan was endorsed by the World Health Assembly in May 2015, with the 193 member states of the United Nations signing a United Nations Political Declaration to take action on antimicrobial resistance in September 2016.118 As part of this declaration, these member states committed to developing national action plans, strategies, and frameworks to address the threat of antimicrobial resistance, based on the Global Action Plan. As one of the member states, Australia released its first antimicrobial resistance strategy, Australia’s First National Antimicrobial Resistance Strategy 2015–2019 in June 2015 which set out the framework and direction for Australia’s response to antimicrobial resistance.119 The strategy was accompanied by the implementation plan Implementation Plan: Australia’s First National Antimicrobial Resistance Strategy 2015–2019 which was released in November 2016 and outlined focus areas for activity,120 and in March 2020 the most current strategy was released, Australia’s National Antimicrobial Resistance Strategy – 2020 and Beyond.121 Building on the objectives outlined in the Global Action Plan, the most recent strategy outlines seven objectives where action is required in Australia:
- Ensure clear governance for antimicrobial resistance initiatives that reflect a shared responsibility between sectors where antimicrobials are used.
- Prevent, reduce, and control infections to prevent the emergence and spread of resistance.
- Improve engagement amongst stakeholders across all sectors, including all members of society, to improve awareness and understanding of the challenge and empower communities to take ownership of the issue.
- Practise effective antimicrobial stewardship and management to reduce the emergence of resistant pathogens.
- Undertake effective and integrated surveillance and threat responses to understand the magnitude, distribution, and impact of resistant organisms.
- Ensure a strong collaborative research agenda across all sectors to support the identification of approaches and techniques to address the antimicrobial resistance threat.
- Strengthen global collaboration and partnerships to influence and contribute to global activities.
Progress against the various initiatives implemented between 2017 and 2019 was reported on in the Final Progress Report: Australia’s First National and Antimicrobial Resistance Strategy 2015–2019, which was released in March 2021.122 This progress report demonstrated that Australia has made significant headway against many of these objectives since the first strategy was released in 2015. Australia’s response has been particularly strong in surveillance of antimicrobial use and resistance, including the establishment of the Antimicrobial Use and Resistance in Australia (AURA) Surveillance System which coordinates data from several sources to provide a comprehensive and integrated picture of antimicrobial use and resistance across Australia, as well as the completion of several antimicrobial resistance surveillance projects in the animal sector. Australia has also implemented various initiatives to strengthen infection prevention and control in both human healthcare settings and in the animal sector, with a focus on developing national evidence-based and best-practice infection prevention and control standards and guidelines. Recognising the global nature of the problem and that the efforts of individual countries is of limited value, Australia has participated in several international surveillance initiatives such as the WHO’s Global Antimicrobial Resistance and Use Surveillance System, as well as leading several collaborative initiatives in the Asia-Pacific region to build capacity in responding to antimicrobial resistance.122
Australia’s approach to date has primarily focused on convening stakeholders and seeking consensus, while leaving the responsibility of implementing and reporting against initiatives to the various players.123 While this approach likely reflects Australia’s complex divisions of authority with multiple levels of government, the lack of centralised governance for the initiatives being undertaken across sectors may be impeding the delivery of an extensive, integrated, and accountable response to antimicrobial resistance and impacting progress against some of the strategic objectives (reported in the latest progress report).
Poor public awareness and understanding of antimicrobial resistance
Several activities have been undertaken to increase awareness and understanding of antimicrobial resistance amongst the public, including education and training programs and campaigns. Several recent studies however have revealed a lack of awareness or knowledge about the proper use of antibiotics and the risks of antimicrobial resistance in Australia.124,125,126,127,128 For example, a nationwide survey published in 2020 revealed that one in five parents reported giving antibiotics to their child without a prescription, and one third of parents would consult another doctor if their initial doctor did not prescribe antibiotics for their children.126 Additionally, several studies indicate that patients underestimate the immediate risk of antimicrobial resistance, with many Australians viewing antimicrobial resistance as a distant issue for future generations.124,129 There are also misconceptions about how antimicrobial resistance occurs, with few understanding how their own behaviours contribute to the development and spread of resistant microbes. Many patients believe that antimicrobial resistance occurs when the body itself becomes resistant to the antimicrobials, and are unaware that resistant microorganisms can be spread between people or from animals to people.130 Additionally, a recent survey performed by the Commonwealth Scientific and Industrial Research Organisation (CSIRO) revealed that 92 per cent of Australian adults do not know the difference between a viral and bacterial infection, with one in four Australians reporting they did not know what antimicrobial resistance is, and one in five believing that antibiotics can be used to treat the common cold.131,132 This lack of awareness leads to inappropriate use of antimicrobials by patients, such as patients retaining unused antibiotics or prescriptions for future self-medicating.130 It may also be resulting in patients placing unnecessary pressure on general practitioners and other medical practitioners to prescribe antimicrobials to meet patient expectations, which could be contributing to the relatively high prescribing rates in Australia.133 Public awareness and understanding of antimicrobial resistance therefore remains a challenge in Australia.
Weaknesses in antimicrobial stewardship practices
Antimicrobial stewardship refers to coordinated actions designed to promote the appropriate prescribing and dispensing of antimicrobials across human and animal health settings.134 The National Centre for Antimicrobial Stewardship is a One Health research programme focused on monitoring the quality of antimicrobial use and implementing antimicrobial stewardship activities to improve this. The centre aims to generate evidence on antimicrobial use and stewardship, influence national policy to promote judicious use of antimicrobials across human and animal health, and improve knowledge and build workforce capacity among all stakeholders.
The National Centre for Antimicrobial Stewardship has had a profound influence on antimicrobial prescribing policy and practice in Australia, facilitating cross sector collaboration to share learnings across all sectors where antimicrobials are used. Overall, Australia has excelled at building and refining a range of programs and initiatives to support effective antimicrobial stewardship in human and animal health settings.135 These antimicrobial stewardship initiatives are largely standard practice in Australian hospitals,134 however implementation remains a challenge in many settings, including regional and rural hospitals, primary care, aged care, animal health and agriculture.135 This is largely due to the absence of strong levers and standards that motivate these settings to implement, maintain and improve stewardship programs, whereas under the National Safety and Quality Health Service Standards Australian hospitals are required to implement antimicrobial stewardship programs. 136
Antimicrobial stewardship programs should encourage collaboration between the manufacturers, prescribers, dispensers, and disposers of antimicrobials. In particular, collaboration between general practitioners as the prescribers and community pharmacists as the dispensers is essential, as general practitioners are the first point of contact to the patient and community pharmacists are well positioned to provide comprehensive medicines advice. While studies show that collaborative stewardship programs between general practitioners and community pharmacists are important to optimising antimicrobial use in primary care, these collaborative programs are currently limited and piecemeal in Australia.137,138,139 This is in part due to a lack of collaborative practice agreements between general practices and community pharmacies, which create a formal relationship between the prescriber and dispenser.139
In addition to collaboration, ensuring that the roles of the manufacturer, prescriber, dispenser, and disposer remain separate is also key to implementing strong stewardship practices in the community, particularly when there is a financial conflict of interest. For example, pharmacists who are responsible for dispensing antimicrobials should not be responsible for prescribing the medication, as there may be a financial incentive to prescribe more medications to increase profits. In those countries with poor separation between roles there is a risk that this conflict of interest may be contributing to poor antimicrobial stewardship practices and higher antimicrobial resistance rates where there is a profit incentive.133,134 While Australia has largely maintained good separation between these various roles, some programs aimed at improving patient access to timely care have created conflicts of interest that may undo the progress Australia has made in implementing good antimicrobial stewardship practices. There have also been programs which propose down-scheduling antimicrobials so they can be prescribed by allied health professionals or available over the counter, which also presents a significant risk to stewardship practices.
Queensland Urinary Tract Infection Pharmacy Pilot
The Queensland Urinary Tract Infection Pharmacy Pilot allows participating pharmacists to prescribe and dispense antibiotics for the treatment of uncomplicated urinary tract infections in non-pregnant women aged 18 to 65. Participating community pharmacists are required to undergo mandatory training to assess, diagnose and treat patients, however there is no requirement for patients to undergo any diagnostic testing.141While this program aims to increase women’s access to care, the conflict of interest between the roles of prescribing and dispensing may have an impact on antimicrobial stewardship practices. It may also make it more challenging to manage patient expectations regarding prescriptions for antimicrobials. Additionally, the antibiotic used in the pilot was trimethoprim, which 23.8 per cent of Escherichia coli were resistant to in 2017, a proportion which is likely to be higher now.142
A similar trial was run in New Zealand in 2012 where trimethoprim could be prescribed and dispensed by trained community pharmacists for the treatment of urinary tract infections. In monitoring the trial, New Zealand’s pharmaceutical management Agency Pharmac noted that there was a steady increase in the number of community dispensed prescriptions for trimethoprim since 2012, although this may reflect the increase in population. Additionally, the Institute of Environmental Science and Research in New Zealand which collects and collates national data on resistance found that the rate of trimethoprim resistance was increasing, although limitations in the data made it difficult to determine whether trimethoprim supplied by pharmacists under the reclassification was directly associated with trimethoprim resistance.143
Poor coordination and incentives in antimicrobial research and development
Australia has a world class research capability and ranks in the top handful of countries globally for biotechnology research innovation. Despite this strong research capability, the lack of a national One Health research agenda for antimicrobial research and development has resulted in poor collaboration and information sharing between research institutes, limited coordination between the various funding streams in Australia,vii and inconsistent allocation of funding across the multiple sectors where antimicrobials are used.122 There has also been poor collaboration with research efforts internationally, which limits the value of the research and results in duplication of effort. These research silos have ultimately resulted in gaps in our understanding of how antimicrobial resistance develops and spreads, and what mechanisms are needed to detect, prevent, and contain it.
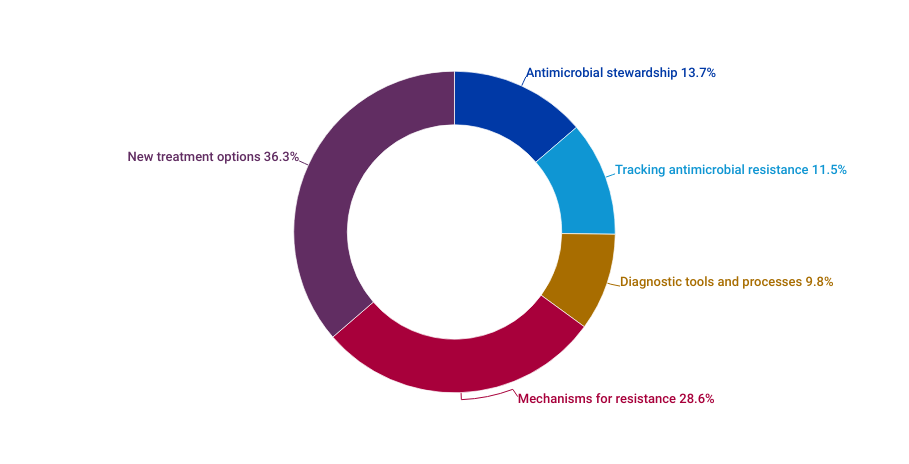
Analysis of the common sources of funding for research related to antimicrobial resistance and the development of novel antimicrobials in Australia reveals that most research is focused on identifying new treatments and targets for new treatments, despite the lack of a viable market for the manufacturing of novel antimicrobials (Figure 7). Australia has limited sovereign manufacturing capability for pharmaceuticals, with 90 per cent of medicines imported.144 This impacts the translation of research into commercial outcomes, as late-stage clinical trials are often required to be conducted overseas, which encourages researchers to pursue their research in other countries instead of Australia. In many cases, Australian researchers will licence their discoveries to pharmaceutical companies overseas because Australia does not have the sovereign capability and infrastructure to manufacture medicines. This means that Australia loses valuable intellectual property, as well as revenue, as the product is commercialised and regulated in the overseas market and then bought back later as the finished product.144
Many countries are exploring ways to improve the antimicrobial market and stimulate investment into antimicrobial research and development to ensure a continuing pipeline of novel therapies. For example, some countries are piloting and implementing alternative reimbursement models which delink reimbursement from the volume of antimicrobials sold to account for the broader value they bring to society.145 While sector leaders have called on government to explore similar initiatives in Australia to incentivise the discovery of new antimicrobials and establish a sovereign manufacturing capability so researchers can manufacture their own discoveries, Australia is still lagging when it comes to translating research into the manufacture of novel antimicrobials.
Uncoordinated governance structures
There are currently two main governance bodies in Australia that are responsible for antimicrobial resistance — the Antimicrobial Resistance Governance Group (ARGG) and the Australian Strategic and Technical Advisory Group on Antimicrobial Resistance (ASTAG). These national bodies also link in with global governance structures, including the Global Leaders Group on Antimicrobial Resistance and the tripartite agencies such as the WHO, the Food and Agriculture Organization of the United Nations (FAO), and the World Organisation for Animal Health (OIE).
The ARGG is the apex governance body that provides national coordination and links between One Health sectors. It has ultimate authority and responsibility for developing and implementing the Australia’s National Antimicrobial Resistance Strategy – 2020 and Beyond and provides input on antimicrobial resistance issues while working with regional, national and international governments across the relevant One Health sectors.
The ASTAG is a multidisciplinary advisory panel comprised of subject matter experts whose purpose is to support the ARGG by providing advice on antimicrobial resistance-related issues. It is also responsible for research priorities and approaches to support implementation of Australia’s National Antimicrobial Resistance Strategy – 2020 and Beyond and Beyond at a national level, with representation across human health, animal health, food, agriculture, and the environment.
In addition to these two main governance structures, the AURA surveillance system is overseen by the Department of Health and Aged Care, and reporting is managed by the Australian Commission on Safety and Quality in Health Care (ACSQHA). The AURA National Coordination Unit (ANCU) of the Commission works with stakeholders to inform action at the local, regional, and national levels to collect and report on antimicrobial use and resistance.
While these national governance structures have been key to various components of the national response (such as the development of the national strategy), many state and territory health, environment, and agriculture departments, as well as organisations and institutions, are not linked into these structures. It is also unclear whether Australia’s governance bodies are linking with global bodies in an effective way. There is currently varying maturity across the One Health sectors, and varying levels of trust towards government institutions. This means that these state and territory government departments, organisations, and institutions are largely operating independently and may make decisions which are not in the interest of the global One Health system. It also means that there is significant duplication of efforts to address antimicrobial resistance.
Positioning Australia as a leader in tackling antimicrobial resistance
Antimicrobial resistance is a global health problem requiring a global response, and one country’s actions will not have a significant impact if other nations continue to act independently of one another. As a wealthy, developed country with an advanced healthcare system, Australia is well placed to lead global efforts to control the growing threat of resistant infections and other health threats, particularly in the Asia-Pacific region. Achieving this will require government to build on the existing work underway and implement initiatives that encourage behavioural change, incentivise antimicrobial research and development, and deliver a unified One Health approach to tackling antimicrobial resistance.
Establishing a Centre for Disease Control
While Australia’s response to the COVID-19 pandemic was successful compared to many other countries, it exposed inconsistencies between states and territories in several areas, including disease tracking, testing capacity, data collection and analysis, vaccine uptake, and communication. This has prompted several organisations, including the AMA, to renew longstanding calls for the establishment of a Centre for Disease Control (CDC), a recognised separate authority for the national scientific leadership and coordination of diseases and health threats.146,147,148
As Australia is the only Organisation for Economic Co-operation and Development (OECD) country without a separate national body to coordinate and control health threats,149 establishing a national CDC will help position Australia as a global leader in tackling diseases and health threats. This could include antimicrobial resistance amongst other health threats such as the current COVID-19 pandemic, future pandemics and communicable diseases, and climate change. Outlined in Figure 8, a CDC would ensure Australia’s response to antimicrobial resistance is coordinated and multifaceted, building on the successful work already underway by integrating existing initiatives and programs into a cohesive national One Health response,ix and linking with various international initiativesx as well as state and territory initiatives
Figure 8: The role for a Centre for Disease Control in leading a One Health approach to address antimicrobial resistance
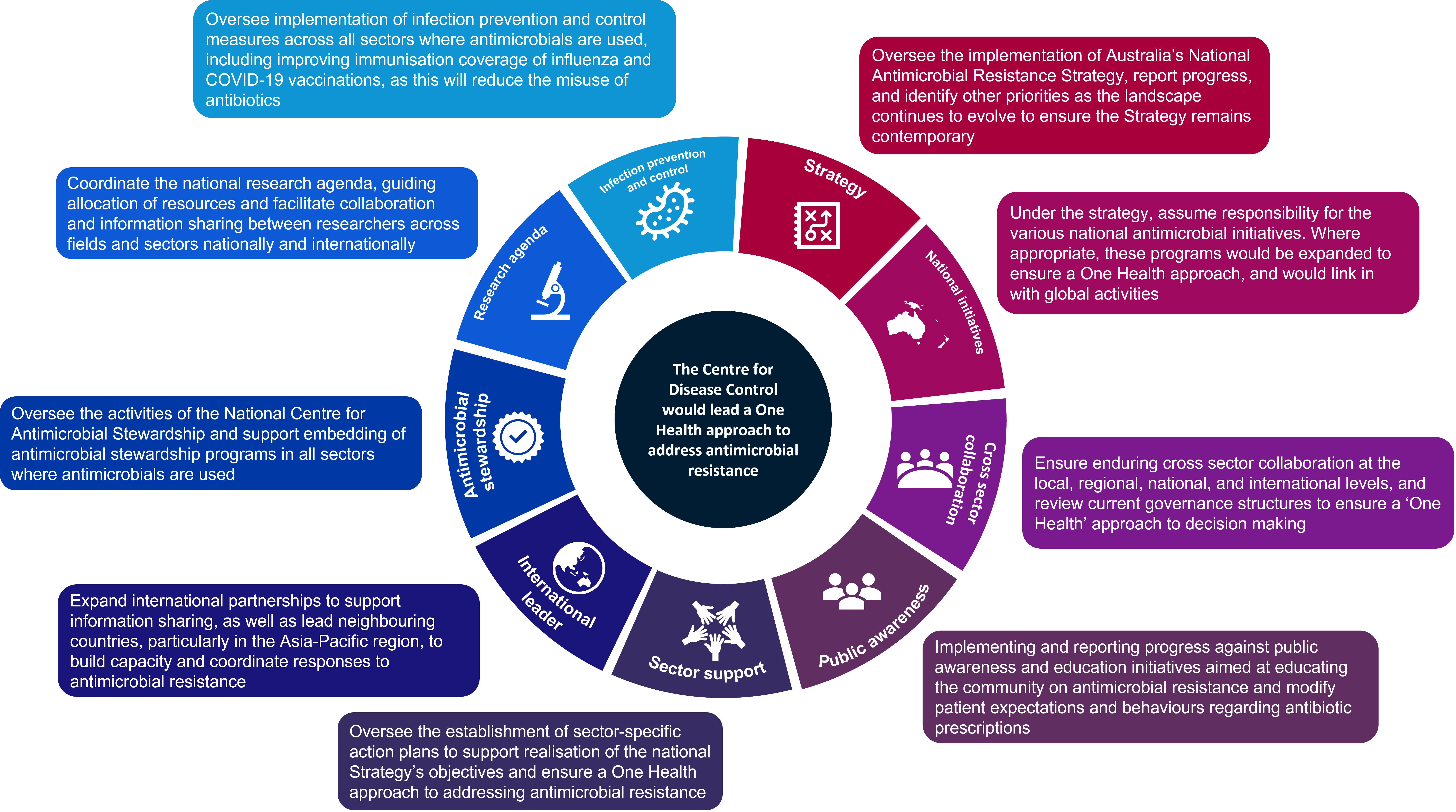
Note: Figure 8 provides an overview of the potential role of a CDC in leading a One Health approach to address antimicrobial resistance. The scope of a CDC would however be broader than antimicrobial resistance and include other health threats such as the current COVID-19 pandemic, future pandemics and communicable diseases, and climate change.
Immediate priorities to be transitioned to a future CDC
Recognising that Australia’s progress against some of the strategic objectives is lagging, there are several immediate priorities that should be addressed now and transitioned to a future CDC to ensure Australia’s response to antimicrobial resistance is effective, integrated, and aligned to One Health objectives.
Review current governance structures to ensure a ‘One Health’ approach to decision making
To achieve the objectives outlined in the strategy, clear lines of responsibility and accountability at the local, regional, national, and global level need to be established, with coordination of effort across the One Health sectors. It is recommended the existing governance structures be reviewed to ensure they are facilitating a One Health approach to decision making at the local, regional, national, and global levels, with effective integration into the role of the CDC. The review should also determine whether the investment in efforts to address antimicrobial resistance are sufficient, sustainable, and responsive to meet the growing threat. It should also determine whether the existing structures are facilitating trust and effective collaboration between the government and other relevant agencies, particularly around the collection, analysis, and sharing of antimicrobial use and resistance data.
Establish sector-specific action plans
Developing, implementing and maintaining sector-specific action plans which outline short-, medium- and long-term goals for each of the One Health sectors will be essential to realising the objectives outlined in the strategy. These sector-specific action plans should be developed following any changes to the governance structure, to ensure there is adequate oversight of the action plans.
Development of a monitoring and evaluation framework
The development of a National One Health Monitoring and Evaluation Framework that measures progress against the strategy’s objectives was outlined in the 2020–21 Federal Budget. While work is currently underway to develop this framework, any changes to the governance arrangements following establishment of the CDC will need to be reflected in this framework. To ensure a One Health focus, the framework should consider how progress against sector-specific plans is monitored and evaluated, and include those actions being taken at the local and regional levels, as opposed to only focusing on national initiatives.
Raise public awareness of antimicrobial resistance
Public awareness and understanding of the correct use of antimicrobials and antimicrobial resistance is essential to driving sustainable consumer behavioural change. While various antimicrobial awareness campaigns and education activities have been implemented in Australia to date, there is an opportunity to better coordinate these activities by developing a One Health communication strategy that will empower consumers to be part of the solution. Building on successful activities implemented to date, the following key messages should be reinforced:
- when antimicrobials should be prescribed, to better manage consumer expectations
- how resistance occurs and spreads, to address current misconceptions
- the harms of antimicrobial resistance and the implications for individuals as well as communities
- the responsibilities consumers have in minimising their contribution to the issue, and the simple steps they can take.
While education resources and campaigns are often targeted at adults and parents, there may be an opportunity to explore whether education on antimicrobial resistance can be better integrated in school curriculum, particularly as many children understand the risks of infectious diseases due to the COVID-19 pandemic.
Coordinate the development of a national One Health research agenda
The development of a national One Health antimicrobial resistance research and development agenda was outlined in the 2020–21 Federal Budget. The development of this agenda will reduce the duplication of effort and silos that currently exist and are limiting the value of Australia’s research. It will also improve the prioritisation of funding across the various sectors to ensure funding is directed to the areas that are critically needed and where it will have the greatest impact. There is an opportunity for the CDC to coordinate the development and/or maintenance of the national research agenda, as the CDC will ensure a One Health approach and regularly engage with stakeholders across the sector to identify where gaps and duplication of effort is occurring and the research areas that need to be prioritised. For example, one of the key reasons cited for increased prescribing is delays in diagnostic tests or cultures and the risk of the infection progressing if timely care is not provided, however this does not appear to be an area that receives significant research funding.
Improving antimicrobial stewardship practices in Australia
Embedding antimicrobial stewardship into all sectors
The National Centre for Antimicrobial Stewardship is undertaking significant work to understand prescribing behaviours across the various sectors where antimicrobials are used, and what strategies are effective at improving the way antimicrobials are used.135 There may be an opportunity for the centre to leverage this existing work, as well as the plethora of stewardship standards, guidelines, recommendations that exist across the various sectors, and develop One Health standards for antimicrobial stewardship.
These One Health standards would detail the role each sector plays in addressing antimicrobial resistance, and the actions each sector needs to take to implement evidence-based stewardship practices to support quality improvement and reduce antimicrobial resistance. This may require a review of existing stewardship guidelines, programs, and tools to ensure they are contemporary, and reflect the specific needs and challenges of each sector. The standards should encourage collaboration between the various sectors and settings to support a One Health approach.
The standards should also facilitate collaboration between the manufacturers, prescribers, dispensers, and disposers of antimicrobials, while ensuring that these roles remain separate, and ensure that appropriate precautions are taken to minimise the emergence and spread of antimicrobial resistance. For example, the Queensland Urinary Tract Infection Pharmacy Pilot and similar pilots pose a significant risk for antimicrobial resistance emergence and spread due to the financial conflict of interest and absence of diagnostic testing, and the standards should ensure a precautionary approach is taken, particularly as the impacts of such pilots on antimicrobial resistance are yet to be established.
To ensure the standards are embedded into all sectors, effectiveness and compliance could be assessed by the National Centre for Antimicrobial Stewardship through the National Antimicrobial Prescribing Survey,150 with opportunities for improvement highlighted to government. This would support the implementation and maintenance of evidence-based and contemporary stewardship practices across all sectors and settings, as well as deliver efficiencies in implementing and monitoring stewardship initiatives. Each sector will also require tailored supports to achieve these standards, and the effectiveness of these supports could be determined and monitored through this survey.
Education and training programs
Enhancing the knowledge of manufacturers, prescribers, dispensers, and disposers of antimicrobials is a key enabler to embedding stewardship into all sectors, as it supports the judicious prescribing, dispensing, and administering of antimicrobials. Efforts to date have largely focused on reinforcing key messages that promote and support appropriate prescribing and knowledge of antimicrobial resistance and stewardship more broadly. There is now an opportunity to consolidate existing knowledge and further shape behavioural change by embedding education and training programs throughout the education, training, and career continuum for those who manufacture, prescribe, dispense, and dispose of antimicrobials. As medical practitioners are responsible for most antimicrobial prescribing, there should be an emphasis on education and training for medical practitioners, including medical students. There may also be an opportunity to develop mechanisms to ‘nudge’ behaviours, such as leveraging the surveillance of antimicrobial use and resistance to raise awareness of local trends.
Clinical decision support and quality improvement
Clinical decision support tools are a key enabler for antimicrobial stewardship, as they can improve adherence to guidelines and standards and therefore optimise antimicrobial prescribing. While such tools have been around for many years in various forms, advances in technology have meant that these tools can now be integrated into clinical software and electronic medical records. While pilots of clinical decision support tools have occurred in Australia, there is an opportunity to expand these systems across the One Health sectors to improve stewardship practices.
Mechanisms to improve the antimicrobial market
Sovereign manufacturing of antimicrobials
Sovereign manufacturing of antimicrobials, as well as other pharmaceuticals, would encourage researchers to undertake antimicrobial discovery and development in Australia, as researchers could retain their intellectual property as opposed to selling them to foreign pharmaceutical companies or venture capitalists. Enabling sovereign manufacturing would enable Australia to remain internationally competitive in antimicrobial research and would help ensure Australia is prepared for future health crises and prevent supply chain issues, as it would enable other critical medicines to be manufactured when required. With the COVID-19 pandemic exposing the risk associated with Australia’s reliance on overseas pharmaceutical manufacturing,144 expanding our sovereign manufacturing capability would be in the national interest while supporting economic growth. A shorter supply chain will also reduce Australia’s carbon footprint, with studies showing supply chains are a significant contributor to carbon emissions. In particular, pharmaceuticals account for 19 per cent of healthcare carbon emissions in Australia, and much of this can likely be attributed to supply chain.
Work is already underway to expand sovereign vaccine manufacturing in Australia,151 and there is an opportunity to expand this capability into other pharmaceuticals such as antimicrobials. Expanding our capability will require a coordinated approach, led by the federal government in collaboration with research organisations, clinicians, pharmaceutical companies, and the biotechnology industry more broadly. It should also be aligned to the Australian Government’s long-term plan for biotechnology in health and medicine Biotechnology in Australia – Strategic Plan for Health and Medicine which was released earlier this year.151
Other mechanisms to incentivise the development of novel antimicrobials
The journey from initial research discovery to a new medicine, therapy or technology is a long one. Usually, the pharmaceutical company is responsible for development, testing, and commercialisation of a medicine, and the significant investment costs are recouped from the product’s subsequent sale. While sovereign manufacturing capability will be a key first step to encouraging antimicrobial research and development, other levers will be required to incentivise pharmaceutical companies to manufacture antimicrobials in Australia (Table 1).
Table 1: Levers to incentivise antimicrobial manufacturing
| Accelerated regulatory approval of antimicrobials | Implementing an accelerated regulatory approval path via the Therapeutics Goods Administration (TGA) for the development of antimicrobials. The US Food and Drug Administration (FDA) offers a similar approval process for drugs or therapies that aim to address a large unmet medical need. |
| Lower tax rates for revenues | Introducing lower tax rates for revenues to create an incentive to manufacture in Australia, as there would be economical societal benefits from manufacturing in Australia. |
| Collaboration between research and industry | Improving collaboration between the research sector and industry to facilitate product development. |
| New reimbursement and procurement models | Establishing new reimbursement and procurement models for pharmaceutical manufacturing to address the market failure. This could include models that assess the value of novel antimicrobials to include the broader value they provide to society. A similar model was piloted in the United Kingdom, whereby the reimbursement was delinked from the volume sold, but rather based on the value to the health system and public health.145 Other reimbursement models could include separate funds for novel antimicrobials other than the PBS, such as a separate Commonwealth insurance fund for novel antimicrobials which evaluates pharmaceuticals on the value they bring to society with respect to treating resistant infections, as opposed to their value for money. |
| Regulatory incentives | Introducing regulatory incentives, such as longer exclusivity periods,xi and waiving of registration fees. |
| Streamlined regulation | Introducing pathways to streamline the regulation process, such as a scheme to facilitate the repurposing of existing drugs or expedite regulation of companion diagnostics,xii adaptation of the orphan drugxiii category to allow for antimicrobials to be considered, or fast-tracked regulation processes specifically for antimicrobials to allow for expedited review. |
Conclusion
Antimicrobial resistance is one of the most serious global public health threats of the 21st century. The economic and human costs are already large enough to justify major intervention, however this threat continues to remain a silent pandemic. Without new antimicrobials, the world may be on track to return to the medical ‘dark ages’, a time where a superficial scratch could be life threatening, and the procedures and treatments which we now rely on are considered too risky to perform, due to the risk of untreatable infection. The solutions proposed in this paper will position Australia as a global leader and support a coordinated, sustained, and unified One Health approach to addressing antimicrobial resistance and other health threats. The need for efficient, effective, and sustainable mechanisms to prevent and treat infectious diseases was clearly demonstrated during the COVID-19 pandemic. Now is the time for strong and sustained action on antimicrobial resistance, as this may well be the cause of the next global pandemic.
Footnotes
i Antimicrobial resistance is commonly discussed in the context of antibiotic resistant bacteria. There are however many other common diseases caused by microorganisms other than bacteria where resistance is occurring, such as HIV which is caused by a virus and malaria which is caused by a parasite. It is for this reason that this report focuses on antimicrobial resistance more broadly.
ii Permafrost is earth material that remains at or below zero degrees Celsius for at least two consecutive years.
iii Australia and the United Kingdom spend about 9 per cent of gross domestic product (GDP) on healthcare.
iv Medical tourism is where patients travel to other countries to obtain medical treatment.
v When determining whether linezolid would be listed on the PBS in 2013
vi Figure 4 depicts the top 10 leading causes of death as a result of non-communicable diseases, disorders and injuries. Communicable diseases were excluded as they are most commonly associated with antimicrobial resistance.
vii Funding streams in Australia include, but are not limited to, Commonwealth government, state and territory governments, private/philanthropic bodies, and international bodies.
viii Analysis of grants awarded through the Medical Research Future Fund, National Health and Medical Research Council, Australian Research Council, Cooperative Research Centre, and Entrepreneurs’ Programme since 2015.
ix Initiatives could include the National Antimicrobial Prescribing Survey, reviewing and updating the Antibacterial Importance Ratings, the online central repository for information relating to antimicrobial resistance www.amr.gov.au, and the Antimicrobial Use and Resistance in Australia (AURA) Surveillance System.
x For example, the World Health Organisation’s Global Antimicrobial Resistance and Use Surveillance System (GLASS)).
xi Exclusivity periods shield prevent competition from any generic versions of a drug which might be developed. Once the exclusivity period expires, other drug manufactures can enter the marker, and can usually lower the price as they do not need to account for large research expenditure. In Australia, exclusivity periods are typically five years, which is often not enough to recoup the development costs.
xii A companion diagnostic is a medical device which provides information that is essential for the safe and effective use of a corresponding drug or biological product.
xiii An orphan drug is a pharmaceutical agent developed to treat medical conditions which, because they are so rare, would not be profitable to produce without government assistance.
References
1 World Health Organisation (2014). Antimicrobial Resistance Global Report on Surveillance. Retrieved 18/05/2022 from: https://apps.who.int/iris/bitstream/handle/10665/112642/9789241564748_eng.pdf?sequence=1&isAllowed=y
2 Wozniak, T.M., Bailey, E.J., & Graves, N. (2019). Health and economic burden of antimicrobial-resistant infections in Australian hospitals: a population-based model. Infection Control & Hospital Epidemiology, 40(3), 320–327. Doi: 10.1017/ICE.2019.2
3 Murray, C.J., Ikuta, K.S., Sharara, F., Swetschinski, L., Robles Aguilar, G., Gray, A., Han, C., Bisignano, C., Rao, P., Wool, E., Johnson, S.C., Browne, A.J., Chipeta, M.G., Fell, F., Hackett, S., Haines-Woodhouse, G., Kashef Hamadani, B.H., Kumaran, E.A.P., McManigal, B., … Naghavi, M. (2022). Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet (London, England), 399(10325), 629. Doi: 10.1016/S0140-6736(21)02724-0
4 Jim O’Neill (2014). Antimicrobial Resistance: Tackling a crisis for the health and wealth of nations. Retrieved 26/05/2022 from: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf
5 Jim O’Neill (2016). Tackling drug-resistant infections globally: final report and recommendations. Retrieved 26/05/2022 from: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf
6 Australian Institute of Health and Welfare (2021). Disease expenditure in Australia 2018-19. Retrieved 16/08/2022 from: https://www.aihw.gov.au/reports/health-welfare-expenditure/disease-expenditure-australia/contents/australian-burden-of-disease-groups
7 Dhammi, I.K., Rehan-Ul-Haq, & Kumar, S. (2015). Prophylactic antibiotics in orthopedic surgery: Controversial issues in its use. Indian Journal of Orthopaedics, 49(4), 373. Doi: 10.4103/0019-5413.159556
8 Herbst, C., Naumann, F., Kruse, E.B., Monsef, I., Bohlius, J., Schulz, H., & Engert, A. (2009). Prophylactic antibiotics or G-CSF for the prevention of infections and improvement of survival in cancer patients undergoing chemotherapy. Cochrane Database of Systematic Reviews, 1. Doi: 10.1002/14651858.CD007107.PUB2
9 Adhikari, B., Pokharel, S., Raut, S., Adhikari, J., Thapa, S., Paudel, K., G C, N., Neupane, S., Neupane, S.R., Yadav, R., Shrestha, S., Rijal, K.R., Marahatta, S.B., Cheah, P.Y., & Pell, C. (2021). Why do people purchase antibiotics over-the-counter? A qualitative study with patients, clinicians and dispensers in central, eastern and western Nepal. BMJ Global Health, 6(5), e005829. Doi: 10.1136/BMJGH-2021-005829
10 Kotwani, A., Joshi, J., & Lamkang, A.S. (2021). Over-the-counter sale of antibiotics in India: A qualitative study of providers’ perspectives across two states. Antibiotics, 10(9), 1123. Doi: 10.3390/ANTIBIOTICS10091123/S1
11 Winstanley, P.A., Ward, S.A., & Snow, R.W. (2002). Clinical status and implications of antimalarial drug resistance. Microbes and Infection, 4(2), 157–164. Doi: 10.1016/S1286-4579(01)01523-4
12 Siltrakool, B., Berrou, I., Griffiths, D., & Alghamdi, S. (2021). Antibiotics’ Use in Thailand: Community Pharmacists’ Knowledge, Attitudes and Practices. Antibiotics 2021, Vol. 10, Page 137, 10(2), 137. Doi: 10.3390/ANTIBIOTICS10020137
13 Geta, K., & Kibret, M. (2022). Knowledge, Attitudes and Practices of Patients on Antibiotic Resistance and Use in Public Hospitals of Amhara Regional State, Northwestern Ethiopia: A Cross-Sectional Study. Infection and Drug Resistance, 15, 193–209. Doi: 10.2147/IDR.S348765
14 Davis, M.E., Liu, T.L., Taylor, Y.J., Davidson, L., Schmid, M., Yates, T., Scotton, J., & Spencer, M.D. (2017). Exploring Patient Awareness and Perceptions of the Appropriate Use of Antibiotics: A Mixed-Methods Study. Antibiotics, 6(4). Doi: 10.3390/ANTIBIOTICS6040023
15 World Health Organization (2015). Antibiotic Resistance: Multi-country public awareness survey. Retrieved 17/08/2022 from: www.who.int
16 Kelesidis, T., & Falagas, M.E. (2015). Substandard/counterfeit antimicrobial drugs. Clinical Microbiology Reviews, 28(2), 443–464. Doi: 10.1128/CMR.00072-14/ASSET/B14ACDE8-06D0-4CF7-9340-B61231FF0000/ASSETS/GRAPHIC/ZCM0021525040002.JPEG
17 Ding, G., Vinturache, A., & Lu, M. (2019). Addressing inappropriate antibiotic prescribing in China. CMAJ : Canadian Medical Association Journal, 191(6), E149. Doi: 10.1503/CMAJ.181417
18 Australian Commission on Safety and Quality in Heath Care (2020). Antimicrobial medicines dispensing from 2013–14 to 2017–18. Retrieved 05/07/2022 from: https://www.safetyandquality.gov.au/our-work/healthcare-variation/antimicrobial-medicines-dispensing-2013-14-2017-18
19 European Centre for Disease Prevention and Control (2019). Surveillance Report: Antimicrobial consumption in the EU/EEA. Retrieved 05/07/2022 from: https://www.ecdc.europa.eu/sites/default/files/documents/Antimicrobial-consumption-EU-EEA.pdf
20 Lum, E.P.M., Page, K., Whitty, J.A., Doust, J., & Graves, N. (2018). Antibiotic prescribing in primary healthcare: Dominant factors and trade-offs in decision-making. Infection, Disease & Health, 23(2), 74–86. Doi: 10.1016/J.IDH.2017.12.002
21 Laka, M., Fellow Adriana Milazzo, R., Lecturer Tracy Merlin, S., & Head, I. (2021). Inappropriate antibiotic prescribing: understanding clinicians’ perceptions to enable changes in prescribing practices. Australian Health Review. Doi: 10.1071/AH21197
22 Lum, E.P.M., Page, K., Nissen, L., Doust, J., & Graves, N. (2017). Australian consumer perspectives, attitudes and behaviours on antibiotic use and antibiotic resistance: a qualitative study with implications for public health policy and practice. BMC Public Health, 17(1). Doi: 10.1186/S12889-017-4813-7
23 Bergen, P.J., Hussainy, S.Y., George, J., Kong, D.C.M., & Kirkpatrick, C.M.J. (2015). Safe disposal of prescribed medicines. Australian Prescriber, 38(3), 90–92. Doi: 10.18773/AUSTPRESCR.2015.031
24 van Boeckel, T.P., Glennon, E.E., Chen, D., Gilbert, M., Robinson, T.P., Grenfell, B.T., Levin, S.A., Bonhoeffer, S., & Laxminarayan, R. (2017). Reducing antimicrobial use in food animals. Science, 357(6358), 1350–1352. Doi: 10.1126/SCIENCE.AAO1495/SUPPL_FILE/AAO1496-VANBOECKEL-SM.PDF
25 Freya Langham, & Allen C Cheng. (2019). Antibiotic use in animals and humans in Australia. Med J Aust , 211(4), 159–160. Doi: 10.5694/mja2.50258
26 Lamichhane, J.R., Osdaghi, E., Behlau, F., Köhl, J., Jones, J.B., & Aubertot, J.N. (2018). Thirteen decades of antimicrobial copper compounds applied in agriculture. A review. Agronomy for Sustainable Development 2018 38:3, 38(3), 1–18. Doi: 10.1007/S13593-018-0503-9
27 Schar, D., Klein, E.Y., Laxminarayan, R., Gilbert, M., & van Boeckel, T.P. (2020). Global trends in antimicrobial use in aquaculture. Scientific Reports 2020 10:1, 10(1), 1–9. Doi: 10.1038/s41598-020-78849-3
28 Manyi-Loh, C., Mamphweli, S., Meyer, E., & Okoh, A. (2018). Antibiotic Use in Agriculture and Its Consequential Resistance in Environmental Sources: Potential Public Health Implications. Molecules : A Journal of Synthetic Chemistry and Natural Product Chemistry, 23(4). Doi: 10.3390/MOLECULES23040795
29 Mann, A., Nehra, K., Rana, J.S., & Dahiya, T. (2021). Antibiotic resistance in agriculture: Perspectives on upcoming strategies to overcome upsurge in resistance. Current Research in Microbial Sciences, 2, 100030. Doi: 10.1016/J.CRMICR.2021.100030
30 Mazutti, K., Costa, L.B., Nascimento, L.V., Filho, T.F., Beirão, B.C.B., Júnior, P.C.M., & Maiorka, A. (2016). Effect of colistin and tylosin used as feed additives on the performance, diarrhea incidence, and immune response of nursery pigs. Undefined, 37(4), 1947–1962. Doi: 10.5433/1679-0359.2016V37N4P1947
31 Valiakos, G., & Kapna, I. (2021). Colistin Resistant mcr Genes Prevalence in Livestock Animals (Swine, Bovine, Poultry) from a Multinational Perspective. A Systematic Review. Veterinary Sciences, 8(11). Doi: 10.3390/VETSCI8110265
32 Australian Government Department of Health and Aged Care (2018). Importance Ratings and Summary of Antibacterial Uses in Human and Animal Health in Australia | Antimicrobial resistance. Retrieved 21/08/2022 from: https://www.amr.gov.au/resources/importance-ratings-and-summary-antibacterial-uses-human-and-animal-health-australia
33 Rajkhowa, A., Bailey, K., Hardefeldt, L., Billman-Jacobe, H., Gilkerson, J., & Browning, G. (2020). Animals, agriculture and antimicrobial stewardship. InSight+. Retrieved 18/05/2022 from: https://insightplus.mja.com.au/2020/2/animals-agriculture-and-antimicrobial-stewardship/
34 Monash University (2022). Centre to Impact AMR. Final Report. Antimicrobial Resistance in Australian Supermarket Meats. Retrieved 18/05/2022 from: https://www.ciwf.org.uk/media/7438137/dutch-slower-
35 van Breda, L.K., Dhungyel, O.P., & Ward, M.P. (2018). Antibiotic resistant Escherichia coli in southeastern Australian pig herds and implications for surveillance. Zoonoses and Public Health, 65(1), e1–e7. Doi: 10.1111/ZPH.12402
36 Bean, D.C., Wigmore, S.M., Abdul Momin, M.H.F., & Wareham, D.W. (2020). Polymyxin Resistant Bacteria in Australian Poultry. Frontiers in Sustainable Food Systems, 4, 177. Doi: 10.3389/FSUFS.2020.550318/BIBTEX
37 Cavicchioli, R., Ripple, W.J., Timmis, K.N., Azam, F., Bakken, L.R., Baylis, M., Behrenfeld, M.J., Boetius, A., Boyd, P.W., Classen, A.T., Crowther, T.W., Danovaro, R., Foreman, C.M., Huisman, J., Hutchins, D.A., Jansson, J.K., Karl, D.M., Koskella, B., Mark Welch, D.B., … Webster, N.S. (2019). Scientists’ warning to humanity: microorganisms and climate change. Nature Reviews Microbiology 2019 17:9, 17(9), 569–586. Doi: 10.1038/s41579-019-0222-5
38 Burnham, J.P. (2021). Climate change and antibiotic resistance: a deadly combination. Therapeutic Advances in Infectious Disease, 8, 2049936121991374. Doi: 10.1177/2049936121991374
39 Rodríguez-Verdugo, A., Lozano-Huntelman, N., Cruz-Loya, M., Savage, V., & Yeh, P. (2020). Compounding Effects of Climate Warming and Antibiotic Resistance. IScience, 23(4), 101024. Doi: 10.1016/J.ISCI.2020.101024
40 MacFadden, D.R., McGough, S.F., Fisman, D., Santillana, M., & Brownstein, J.S. (2018). Antibiotic resistance increases with local temperature. Nature Climate Change 2018 8:6, 8(6), 510–514. Doi: 10.1038/s41558-018-0161-6
41 Reverter, M., Sarter, S., Caruso, D., Avarre, J.C., Combe, M., Pepey, E., Pouyaud, L., Vega-Heredía, S., de Verdal, H., & Gozlan, R.E. (2020). Aquaculture at the crossroads of global warming and antimicrobial resistance. Nature Communications 2020 11:1, 11(1), 1–8. Doi: 10.1038/s41467-020-15735-6
42 Rocklöv, J., & Dubrow, R. (2020). Climate change: an enduring challenge for vector-borne disease prevention and control. Nature Immunology, 21(6), 695. Doi: 10.1038/S41590-020-0692-7
43 Andrade, L., O’Dwyer, J., O’Neill, E., & Hynds, P. (2018). Surface water flooding, groundwater contamination, and enteric disease in developed countries: A scoping review of connections and consequences. Environmental Pollution (Barking, Essex : 1987), 236, 540–549. Doi: 10.1016/J.ENVPOL.2018.01.104
44 Byers, J.E. (2020). Effects of climate change on parasites and disease in estuarine and nearshore environments. PLoS Biology, 18(11). Doi: 10.1371/JOURNAL.PBIO.3000743
45 MacFadden, D.R., McGough, S.F., Fisman, D., Santillana, M., & Brownstein, J.S. (2018). Antibiotic resistance increases with local temperature. Nature Climate Change 2018 8:6, 8(6), 510–514. Doi: 10.1038/s41558-018-0161-6
46 McGough, S.F., MacFadden, D.R., Hattab, M.W., Mølbak, K., & Santillana, M. (2020). Rates of increase of antibiotic resistance and ambient temperature in Europe: a cross-national analysis of 28 countries between 2000 and 2016. Eurosurveillance, 25(45), 1–12. Doi: 10.2807/1560-7917.ES.2020.25.45.1900414
47 Kim, H., Kim, M., Kim, S., Lee, Y.M., & Shin, S.C. (2022). Characterization of antimicrobial resistance genes and virulence factor genes in an Arctic permafrost region revealed by metagenomics. Environmental Pollution, 294, 118634. Doi: 10.1016/J.ENVPOL.2021.118634
48 Segawa, T., Takeuchi, N., Rivera, A., Yamada, A., Yoshimura, Y., Barcaza, G., Shinbori, K., Motoyama, H., Kohshima, S., & Ushida, K. (2013). Distribution of antibiotic resistance genes in glacier environments. Environmental Microbiology Reports, 5(1), 127–134. Doi: 10.1111/1758-2229.12011
49 Schuur, E.A.G., McGuire, A.D., Schädel, C., Grosse, G., Harden, J.W., Hayes, D.J., Hugelius, G., Koven, C.D., Kuhry, P., Lawrence, D.M., Natali, S.M., Olefeldt, D., Romanovsky, V.E., Schaefer, K., Turetsky, M.R., Treat, C.C., & Vonk, J.E. (2015). Climate change and the permafrost carbon feedback. Nature 2015 520:7546, 520(7546), 171–179. Doi: 10.1038/nature14338
50 Malik, A., Lenzen, M., McAlister, S., & McGain, F. (2018). The carbon footprint of Australian health care. The Lancet Planetary Health, 2(1), e2–e3. Doi: 10.1016/S2542-5196
51 Climate Council (2021, March 18). Climate Council Welcomes Call For Net Zero Health Sector. Retrieved 25/08/2022 from: https://www.climatecouncil.org.au/resources/net-zero-health-sector/
52 Doctors for the Environment Australia (2020). Net zero carbon emissions: responsibilities, pathways and opportunities for Australia’s healthcare sector. Retrieved 25/08/2022 from: https://www.dea.org.au/wp-content/uploads/2020/12/DEA-Net-Zero-report_v11.pdf
53 Climate and Health Alliance (2021, April 16). Health sector gets first-ever guide to reach zero greenhouse gas emissions by 2050. Retrieved 25/08/2022 from: https://www.caha.org.au/healthcare_decarbonisation
54 Australian Medical Association, & Doctors for the Environment Australia (2021, March 18). Joint statement - Medical professionals call for emissions reduction in health care. 627. Doi: 10.1016/j.scitotenv.2018.01.193
55 Australian Medical Association (2019). Environmental Sustainability in Health Care - 2019. Retrieved 25/08/2022 from: https://www.ama.com.au/position-statement/environmental-sustainability-health-care-2019
56 Milner, J., Hamilton, I., Woodcock, J., Williams, M., Davies, M., Wilkinson, P., & Haines, A. (2020). Health benefits of policies to reduce carbon emissions. BMJ, 368. Doi: 10.1136/BMJ.L6758
57 Hofer, U. (2021). Rise in global antibiotic use. Nature Reviews Microbiology 2021 20:2, 20(2), 63–63. Doi: 10.1038/s41579-021-00668-8
58 Klein, E.Y., van Boeckel, T.P., Martinez, E.M., Pant, S., Gandra, S., Levin, S.A., Goossens, H., & Laxminarayan, R. (2018). Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proceedings of the National Academy of Sciences of the United States of America, 115(15), E3463–E3470. Doi: 10.1073/PNAS.1717295115
59 Sridhar, S., Turbett, S.E., Harris, J.B., & LaRocque, R.C. (2021). Antimicrobial-resistant bacteria in international travelers. Current Opinion in Infectious Diseases, 34(5), 423. Doi: 10.1097/QCO.0000000000000751
60 Sridhar, S., Turbett, S.E., Harris, J.B., & LaRocque, R.C. (2021). Antimicrobial-resistant bacteria in international travelers. Current Opinion in Infectious Diseases, 34(5), 423. Doi: 10.1097/QCO.0000000000000751
61 Kennedy, K., & Collignon, P. (2010). Colonisation with Escherichia coli resistant to “critically important” antibiotics: a high risk for international travellers. European Journal of Clinical Microbiology & Infectious Diseases : Official Publication of the European Society of Clinical Microbiology, 29(12), 1501–1506. Doi: 10.1007/S10096-010-1031-Y
62 Chua, K.Y.L., Lindsay Grayson, M., Burgess, A.N., Lee, J.Y.H., & Howden, B.P. (2014). The growing burden of multidrug-resistant infections among returned Australian travellers. The Medical Journal of Australia, 200(2), 116–118. Doi: 10.5694/MJA13.10592
63 Benenson, S., Nir-Paz, R., Golomb, M., Schwartz, C., Amit, S., Moses, A.E., & Cohen, M.J. (2018). Carriage of multi-drug resistant bacteria among foreigners seeking medical care. Scientific Reports, 8(1). Doi: 10.1038/S41598-018-27908-X
64 Khuntayaporn, P., Kanathum, P., Houngsaitong, J., Montakantikul, P., Thirapanmethee, K., & Chomnawang, M.T. (2021). Predominance of international clone 2 multidrug-resistant Acinetobacter baumannii clinical isolates in Thailand: a nationwide study. Annals of Clinical Microbiology and Antimicrobials, 20(1), 1–11. Doi: 10.1186/S12941-021-00424-Z
65 Kumarasamy, K.K., Toleman, M.A., Walsh, T.R., Bagaria, J., Butt, F., Balakrishnan, R., Chaudhary, U., Doumith, M., Giske, C.G., Irfan, S., Krishnan, P., Kumar, A. v., Maharjan, S., Mushtaq, S., Noorie, T., Paterson, D.L., Pearson, A., Perry, C., Pike, R., … Woodford, N. (2010). Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study. The Lancet. Infectious Diseases, 10(9), 597. Doi: 10.1016/S1473-3099(10)70143-2
66 Mohamed Naeemmudeen, N., Ainaa Nabihah Mohd Ghazali, N., Bahari, H., Ibrahim, R., Dzulfikar Samsudin, A., & Syawani Jasni, A. (n.d.-bn). Trends in antimicrobial resistance in Malaysia.
67 Probyn, E., Jones, M., Bell, D., Sanchez Taylor, J., Hunter, E., Cheunha, O., & Cho, J.H. (2014). Sun, Sea, Sand and SIlicone. Mapping Cosmetic Surgery Tourism. Final Report. Retrieved 19/08/2022 from: https://eprints.whiterose.ac.uk/80613/1/Sun%20Sea%20Final%20Report.pdf
68 World Health Organization (2021). Global antimicrobial resistance and use surveillance system (GLASS) report 2021. In World Health Organization. Retrieved 22/08/2022 from: http://www.who.int/glass/resources/publications/early-implementation-report-2020/en/
69 Choudhury, S., Medina-Lara, A., & Smith, R. (2022). Antimicrobial resistance and the COVID-19 pandemic. Bulletin of the World Health Organization, 100(5), 295. Doi: 10.2471/BLT.21.287752
70 Silver, L.L. (2011). Challenges of antibacterial discovery. Clinical Microbiology Reviews, 24(1), 71–109. Doi: 10.1128/CMR.00030-10
71 Darrow, J.J., Sinha, M.S., & Kesselheim, A.S. (2018). When markets fail: Patents and infectious disease products. Food and Drug Law Journal, 73(3), 361–382.
72 Spellberg, B. (2014). The future of antibiotics. Critical Care, 18(3), 1–7. Doi: 10.1186/CC13948/FIGURES/1
73 Todd, M.H., Klug, D.M., Idiris, F.I.M., Blaskovich, M.A.T., von Delft, F., Dowson, C.G., Kirchhelle, C., Roberts, A.P., & Singer, A.C. (2021). There is no market for new antibiotics: this allows an open approach to research and development. Wellcome Open Research, 6. Doi: 10.12688/WELLCOMEOPENRES.16847.1
74 Plackett, B. (2020). Why big pharma has abandoned antibiotics. Nature, 586(7830), S50–S52. Doi: 10.1038/D41586-020-02884-3
75 Towse, A., Hoyle, C.K., Goodall, J., Hirsch, M., Mestre-Ferrandiz, J., & Rex, J.H. (2017). Time for a change in how new antibiotics are reimbursed: Development of an insurance framework for funding new antibiotics based on a policy of risk mitigation. Health Policy (Amsterdam, Netherlands), 121(10), 1025–1030. Doi: 10.1016/J.HEALTHPOL.2017.07.011
76 Thomas, D., & Wessel, C. (2022). The State of Innovation in Antibacterial Therapeutics. Retrieved 04/06/2022 from: https://www.bio.org/sites/default/files/2022-02/The-State-of-Innovation-in-Antibacterial-Therapeutics.pdf
77 Australian Government Department of Health and Aged Care (2013). Pharmaceutical Benefits Scheme: Linezolid, injection, 600 mg per 300 mL, tablet, 600 mg and powder for oral suspension, 20 mg per mL, Zyvox® - July 2013. Retrieved 25/08/2022 from: https://www.pbs.gov.au/info/industry/listing/elements/pbac-meetings/psd/2013-07/linezolid
78 Manyi-Loh, C., Mamphweli, S., Meyer, E., & Okoh, A. (2018). Antibiotic Use in Agriculture and Its Consequential Resistance in Environmental Sources: Potential Public Health Implications. Molecules: A Journal of Synthetic Chemistry and Natural Product Chemistry, 23(4). Doi: 10.3390/MOLECULES23040795
79 Kraemer, S.A., Ramachandran, A., & Perron, G.G. (2019). Antibiotic Pollution in the Environment: From Microbial Ecology to Public Policy. Microorganisms, 7(6). Doi: 10.3390/MICROORGANISMS7060180
80 Haberecht, H.B., Nealon, N.J., Gilliland, J.R., Holder, A. v., Runyan, C., Oppel, R.C., Ibrahim, H.M., Mueller, L., Schrupp, F., Vilchez, S., Antony, L., Scaria, J., & Ryan, E.P. (2019). Antimicrobial-Resistant Escherichia coli from Environmental Waters in Northern Colorado. Journal of Environmental and Public Health, 2019. Doi: 10.1155/2019/3862949
81 Hembach, N., Schmid, F., Alexander, J., Hiller, C., Rogall, E.T., & Schwartz, T. (2017). Occurrence of the mcr-1 colistin resistance gene and other clinically relevant antibiotic resistance genes in microbial populations at different municipal wastewater treatment plants in Germany. Frontiers in Microbiology, 8(JUL), 1282. Doi: 10.3389/FMICB.2017.01282/BIBTEX
82 Laxminarayan, R., & Chaudhury, R.R. (2016). Antibiotic Resistance in India: Drivers and Opportunities for Action. PLoS Medicine, 13(3). Doi: 10.1371/JOURNAL.PMED.1001974
83 Changing Markets, & Ecostorm. (2016). Superbugs in the supply chain: how pollution from antibiotics factories in India and China is fuelling the global rise of drug-resistant infections. Retrieved 30/08/2022 from: https://epha.org/wp-content/uploads/2016/10/Superbugsinthesupplychain_CMreport.pdf
84 Ekundayo, T.C., & Okoh, A.I. (2020). Antimicrobial resistance in freshwater Plesiomonas shigelloides isolates: Implications for environmental pollution and risk assessment. Environmental Pollution, 257, 113493. Doi: 10.1016/J.ENVPOL.2019.113493
85 Grenni, P., Ancona, V., & Barra Caracciolo, A. (2018). Ecological effects of antibiotics on natural ecosystems: A review. Microchemical Journal, 136, 25–39. Doi: 10.1016/J.MICROC.2017.02.006
86 Perera, L.N., Mafiz, A.I., Amarasekara, N.R., Chang, E., Krishnoji Rao, V.B., & Zhang, Y. (2020). Antimicrobial-resistant E. coli and Enterococcus spp. Recovered from urban community gardens. Food Control, 108, 106857. Doi: 10.1016/J.FOODCONT.2019.106857
87 Bennani, H., Mateus, A., Mays, N., Eastmure, E., Stärk, K.D.C., & Häsler, B. (2020). Overview of Evidence of Antimicrobial Use and Antimicrobial Resistance in the Food Chain. Antibiotics 2020, Vol. 9, Page 49, 9(2), 49. Doi: 10.3390/ANTIBIOTICS9020049
88 Thapa, S.P., Shrestha, S., & Anal, A.K. (2020). Addressing the antibiotic resistance and improving the food safety in food supply chain (farm-to-fork) in Southeast Asia. Food Control, 108, 106809. Doi: 10.1016/J.FOODCONT.2019.106809
89 Alawi, M., Torrijos, T.V., & Walsh, F. (2022). Plasmid-mediated antimicrobial resistance in drinking water. Environmental Advances, 8, 100191. Doi: 10.1016/J.ENVADV.2022.100191
90 United Nations Environment Programme (2017). Frontiers 2017: Emerging Issues of Environmental Concern. Retrieved 30/08/2022 from: https://www.unep.org/resources/frontiers-2017-emerging-issues-environmental-concern
91 Pérez de la Lastra, J.M., Anand, U., González-Acosta, S., López, M.R., Dey, A., Bontempi, E., & Morales delaNuez, A. (2022). Antimicrobial Resistance in the COVID-19 Landscape: Is There an Opportunity for Anti-Infective Antibodies and Antimicrobial Peptides? Frontiers in Immunology, 0, 2698. Doi: 10.3389/FIMMU.2022.921483
92 Knight, G.M., Glover, R.E., McQuaid, C.F., Olaru, I.D., Gallandat, K., Leclerc, Q.J., Fuller, N.M., Willcocks, S.J., Hasan, R., van Kleef, E., & Chandler, C.I.R. (2021). Antimicrobial resistance and covid-19: Intersections and implications. ELife, 10, 1–27. Doi: 10.7554/ELIFE.64139
93 Afshinnekoo, E., Bhattacharya, C., Burguete-GarcÃ, A., Castro-Nallar, E., Deng, Y., Desnues, C., Dias-Neto, E., Elhaik, E., Iraola, G., Jang, S., Å, P.P., Mason, C.E., Nagarajan, N., Poulsen, M., Prithiviraj, B., Siam, R., Shi, T., Suzuki, H., Werner, J., … Consortium, M. (2021). COVID-19 drug practices risk antimicrobial resistance evolution. Doi: 10.1016/S2666-5247(21)00039-2
94 Adebisi, Y.A., Alaran, A.J., Okereke, M., Oke, G.I., Amos, O.A., Olaoye, O.C., Oladunjoye, I., Olanrewaju, A.Y., Ukor, N.A., & Lucero-Prisno, D.E. (2021). COVID-19 and Antimicrobial Resistance: A Review. Infectious Diseases, 14, 117863372110338. Doi: 10.1177/11786337211033870
95 Pelfrene, E., Botgros, R., & Cavaleri, M. (2021). Antimicrobial multidrug resistance in the era of COVID-19: a forgotten plight? Antimicrobial Resistance and Infection Control, 10(1), 1–6. Doi: 10.1186/S13756-021-00893-Z
96 Ramay, B.M., Caudell, M.A., Cordón-Rosales, C., Archila, L.D., Palmer, G.H., Jarquin, C., Moreno, P., McCracken, J.P., Rosenkrantz, L., Amram, O., Omulo, S., & Call, D.R. (2020). Antibiotic use and hygiene interact to influence the distribution of antimicrobial-resistant bacteria in low-income communities in Guatemala. Scientific Reports 2020 10:1, 10(1), 1–10. Doi: 10.1038/s41598-020-70741-4
97 Pokharel, S., Raut, S., & Adhikari, B. (2019). Tackling antimicrobial resistance in low-income and middle-income countries. BMJ Global Health, 4(6), e002104. Doi: 10.1136/BMJGH-2019-002104
98 Fink, G., D’Acremont, V., Leslie, H.H., & Cohen, J. (2020). Antibiotic exposure among children younger than 5 years in low-income and middle-income countries: a cross-sectional study of nationally representative facility-based and household-based surveys. The Lancet Infectious Diseases, 20(2), 179–187. Doi: 10.1016/S1473-3099(19)30572-9
99 Sartelli, M., Hardcastle, T.C., Catena, F., Chichom-Mefire, A., Coccolini, F., Dhingra, S., Haque, M., Hodonou, A., Iskandar, K., Labricciosa, F.M., Marmorale, C., Sall, I., & Pagani, L. (2020). Antibiotic Use in Low and Middle-Income Countries and the Challenges of Antimicrobial Resistance in Surgery. Antibiotics, 9(8), 1–12. Doi: 10.3390/ANTIBIOTICS9080497
100 Mingeot-Leclercq, M.P., & Tulkens, P.M. (1999). Aminoglycosides: Nephrotoxicity. Antimicrobial Agents and Chemotherapy, 43(5), 1003. Doi: 10.1128/AAC.43.5.1003
101 Selimoglu, E. (2007). Aminoglycoside-induced ototoxicity. Current Pharmaceutical Design, 13(1), 119–126. Doi: 10.2174/138161207779313731
102 Peres-Bota, D., Rodriguez, H., Dimopoulos, G., DaRos, A., Mélot, C., Struelens, M.J., & Vincent, J.L. (2003). Are infections due to resistant pathogens associated with a worse outcome in critically ill patients? Journal of Infection, 47(4), 307–316. Doi: 10.1016/S0163-4453(03)00100-2
103 Seddon, J.A., Godfrey-Faussett, P., Jacobs, K., Ebrahim, A., Hesseling, A.C., & Schaaf, H.S. (2012). Hearing loss in patients on treatment for drug-resistant tuberculosis. European Respiratory Journal, 40(5), 1277–1286. Doi: 10.1183/09031936.00044812
104 Osborne, J., Paget, J., Paget, J., Giles-Vernick, T., Kutalek, R., Rodyna, R., Ahmed, S.M., & Dückers, M. (2021). Addressing vulnerabilities in communities facing infectious disease threats: A need for social science-driven assessments. Journal of Global Health, 11, 1–4. Doi: 10.7189/JOGH.11.03003
105 Global Burden of Disease Collaborative Network (2021). Global Burden of Disease Study 2019 (GBD 2019). Institute for Health Metrics and Evaluation (IHME). Retrieved 26/08/2022 from: https://www.healthdata.org/gbd/2019
106 Geneva: World Health Organization (2021). HIV drug resistance report 2022. Retrieved 26/08/2022 from: https://www.who.int/publications/i/item/9789240038608
107 Balikagala, B., Fukuda, N., Ikeda, M., Katuro, O.T., Tachibana, S.-I., Yamauchi, M., Opio, W., Emoto, S., Anywar, D.A., Kimura, E., Palacpac, N.M.Q., Odongo-Aginya, E.I., Ogwang, M., Horii, T., & Mita, T. (2021). Evidence of Artemisinin-Resistant Malaria in Africa. New England Journal of Medicine, 385(13), 1163–1171. Doi: 10.1056/NEJMOA2101746
108 Geneva: World Health Organization (2021). World malaria report 2021. Retrieved 26/08/2022 from: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2021
109 Tong, S. Y., van Hal, S. J., Einsiedel, L., Currie, B. J., & Turnidge, J. D. (2012). Impact of ethnicity and socio-economic status on Staphylococcus aureus bacteremia incidence and mortality: a heavy burden in indigenous Australians. BMC infectious diseases, 12(1), 1-9. Doi: https://doi.org/10.1186/1471-2334-12-249
110 Thorpe, K.E., Joski, P., & Johnston, K.J. (2018). Antibiotic-resistant infection treatment costs have doubled since 2002, now exceeding $2 billion annually. Health Affairs, 37(4), 662–669. Doi: 10.1377/HLTHAFF.2017.1153
111 Roberts, R.R., Hota, B., Ahmad, L., Scott, D., Foster, S.D., Abbasi, F., Schabowski, S., Kampe, L.M., Gr-Ciavarella, G., Supino, M., Naples, J., Cordell, R., Levy, S.B., & Weinstein, R.A. (2009). Hospital and societal costs of antimicrobial-resistant infections in a chicago teaching hospital: implications for antibiotic stewardship. Clinical Infectious Diseases, 49(8), 1175–1184. Doi: 10.1086/605630/2/49-8-1175-FIG002.GIF
112 Mauldin, P.D., Salgado, C.D., Hansen, I.S., Durup, D.T., & Bosso, J.A. (2010). Attributable hospital cost and length of stay associated with health care-associated infections caused by antibiotic-resistant gram-negative bacteria. Antimicrobial Agents and Chemotherapy, 54(1), 109–115. Doi: 10.1128/AAC.01041-09
113 Touat, M., Opatowski, M., Brun-Buisson, C., Cosker, K., Guillemot, D., Salomon, J., Tuppin, P., de Lagasnerie, G., & Watier, L. (2019). A Payer Perspective of the Hospital Inpatient Additional Care Costs of Antimicrobial Resistance in France: A Matched Case–Control Study. Applied Health Economics and Health Policy, 17(3), 381–389. Doi: 10.1007/S40258-018-0451-1
114 Outbreak Consortium (2020). Superbugs to trigger our next Global Financial Crisis. Retrieved 23/08/2022 from: https://outbreakproject.com.au/2020/04/22/superbugs-to-trigger-our-next-global-financial-crisis/
115 KPMG (2014). The global economic impact of anti-microbial resistance. Retrieved 11/09/2022 from: https://assets.kpmg/content/dam/kpmg/pdf/2014/12/amr-report-final.pdf
116 Ahmed, S.A., Baris, E., Go, D.S., Lofgren, H., Osorio-Rodarte, I., & Thierfelder, K. (2017). Assessing the Global Economic and Poverty Effects of Antimicrobial Resistance. Assessing the Global Economic and Poverty Effects of Antimicrobial Resistance. Doi: 10.1596/1813-9450-8133
117 World Health Organization (2015). Global Action Plan on Antimicrobial Resistance. In Microbe Magazine (Vol. 10, Issue 9). Retrieved 23/08/2022 from: https://www.who.int/publications/i/item/9789241509763
118 United Nations (2016). Political declaration of the high-level meeting of the General Assembly on antimicrobial resistance: draft resolution/submitted by the President of the General Assembly. Retrieved 23/08/2022 from: https://digitallibrary.un.org/record/842813?ln=en#record-files-collapse-header
119 Commonwealth of Australia (2015). National Antimicrobial Resistance Strategy 2015-2019. Retrieved 23/08/2022 from: https://www.amr.gov.au/resources/national-amr-strategy
120 Commonwealth of Australia (2016). Implementation Plan: Australia’s First National Antimicrobial Resistance Strategy 2015–2019 | Antimicrobial resistance. Retrieved 23/08/2022 from: https://www.amr.gov.au/resources/national-amr-implementation-plan
121 Commonwealth of Australia (2020). Australia’s National Antimicrobial Resistance Strategy – 2020 and Beyond . Retrieved 23/08/2022 from: https://www.amr.gov.au/resources/australias-national-antimicrobial-resistance-strategy-2020-and-beyond
122 Commonwealth of Australia (2021). Final Progress Report: Australia’s First National Antimicrobial Resistance Strategy 2015–2019 | Antimicrobial resistance. Retrieved 23/08/2022 from: https://www.amr.gov.au/resources/final-progress-report-australias-first-national-antimicrobial-resistance-strategy-2015
123 Hannah, A., & Baekkeskov, E. (2020). The promises and pitfalls of polysemic ideas: ‘One Health’ and antimicrobial resistance policy in Australia and the UK. Policy Sciences 2020 53:3, 53(3), 437–452. Doi: 10.1007/S11077-020-09390-3
124 Alejandro, A.L., Bruce, M., & Leo, C. (2022). Parents’ awareness of antimicrobial resistance: a qualitative study utilising the Health Belief Model in Perth, Western Australia. Australian and New Zealand Journal of Public Health. Doi: 10.1111/1753-6405.13265
125 Bosley, H., Henshall, C., Appleton, J. v., & Jackson, D. (2018). A systematic review to explore influences on parental attitudes towards antibiotic prescribing in children. Journal of Clinical Nursing, 27(5–6), 892–905. Doi: 10.1111/JOCN.14073
126 Anderson, R., Rhodes, A., Cranswick, N., Downes, M., O’Hara, J., Measey, M.A., & Gwee, A. (2020). A nationwide parent survey of antibiotic use in Australian children. The Journal of Antimicrobial Chemotherapy, 75(5), 1347–1351. Doi: 10.1093/JAC/DKZ448
127 Bakhit, M., del Mar, C., Gibson, E., & Hoffmann, T. (2019). Exploring patients’ understanding of antibiotic resistance and how this may influence attitudes towards antibiotic use for acute respiratory infections: a qualitative study in Australian general practice. BMJ Open, 9(3), e026735. Doi: 10.1136/BMJOPEN-2018-026735
128 Davis, M.D.M., Lohm, D.B., Whittaker, A., & Flowers, P. (2020). “Willy nilly” doctors, bad patients, and resistant bodies in general public explanations of antimicrobial resistance. Sociology of Health & Illness, 42(6), 1394–1408. Doi: 10.1111/1467-9566.13111
129 Langford, B.J., Daneman, N., Leung, V., Wu, J.H.C., Brown, K., Schwartz, K.L., & Garber, G. (2019). The second-hand effects of antibiotics: communicating the public health risks of drug resistance. JAC-Antimicrobial Resistance, 1(3). Doi: 10.1093/JACAMR/DLZ059
130 Lum, E.P.M., Page, K., Nissen, L., Doust, J., & Graves, N. (2017). Australian consumer perspectives, attitudes and behaviours on antibiotic use and antibiotic resistance: a qualitative study with implications for public health policy and practice. BMC Public Health, 17(1). Doi: 10.1186/S12889-017-4813-7
131 Paul De Barro (2020, March 15). ‘Deeply worrying’: 92% of Australians don’t know the difference between viral and bacterial infections. The Conversation.
132 Outbreak Project (2020). Public information key to combatting rising superbug threat. Retrieved 04/07/2022 from: https://outbreakproject.com.au/2020/05/14/public-information-key-to-combatting-rising-superbug-threat/
133 Lum, E.P.M., Page, K., Whitty, J.A., Doust, J., & Graves, N. (2018). Antibiotic prescribing in primary healthcare: Dominant factors and trade-offs in decision-making. Infection, Disease & Health, 23(2), 74–86. Doi: 10.1016/J.IDH.2017.12.002
134 Australian Commission on Safety and Quality in Health Care (2022). Antimicrobial stewardship. Retrieved 23/08/2022 from: https://www.safetyandquality.gov.au/standards/nsqhs-standards/preventing-and-controlling-infections-standard/antimicrobial-stewardship
135 Thursky, K.A., Hardefeldt, L.Y., Rajkhowa, A., Ierano, C., Bishop, J., Hawes, L., Biezen, R., Saha, S.K., Dowson, L., Bailey, K.E., Scarborough, R., Little, S.B., Gotterson, F., Hur, B., Khanina, A., Urbancic, K., Crabb, H.K., Richards, S., Sri, A., … Koning, S. (2021). Antimicrobial stewardship in Australia: the role of qualitative research in programme development. JAC-Antimicrobial Resistance, 3(4). Doi: 10.1093/JACAMR/DLAB166
136 Australian Commission on Safety and Quality in Health Care (2022). The NSQHS Standards. Retrieved 23/08/2022 from: https://www.safetyandquality.gov.au/standards/nsqhs-standards
137 Saha, S.K., Kong, D.C.M., Thursky, K., & Mazza, D. (2020). A Nationwide Survey of Australian General Practitioners on Antimicrobial Stewardship: Awareness, Uptake, Collaboration with Pharmacists and Improvement Strategies. Antibiotics, 9(6), 1–13. Doi: 10.3390/ANTIBIOTICS9060310
138 Saha, S.K., Kong, D.C.M., Thursky, K., & Mazza, D. (2021). Divergent and Convergent Attitudes and Views of General Practitioners and Community Pharmacists to Collaboratively Implement Antimicrobial Stewardship Programs in Australia: A Nationwide Study. Antibiotics, 10(1), 1–18. Doi: 10.3390/ANTIBIOTICS10010047
139 Saha, S.K., Kong, D.C.M., Thursky, K., & Mazza, D. (2021). Development of an antimicrobial stewardship implementation model involving collaboration between general practitioners and pharmacists: GPPAS study in Australian primary care. Primary Health Care Research & Development, 22. Doi: 10.1017/S1463423620000687
140 Shet, A., Sundaresan, S., & Forsberg, B.C. (2015). Pharmacy-based dispensing of antimicrobial agents without prescription in India: Appropriateness and cost burden in the private sector. Antimicrobial Resistance and Infection Control, 4(1), 1–7. Doi: 10.1186/S13756-015-0098-8
141 Lisa Nissen, Esther Lau, & Jean Spinks. (2022). The management of urinary tract infections by community pharmacists: A state-wide trial : Urinary Tract Infection Pharmacy Pilot - Queensland (Outcome Report). Retrieved 23/08/2022 from: https://eprints.qut.edu.au/232923/1/UTIPP_Q_Final_Report_2022_QUT_for_publication.pdf
142 Ny, S., Edquist, P., Dumpis, U., Gröndahl-Yli-Hannuksela, K., Hermes, J., Kling, A.M., Klingeberg, A., Kozlov, R., Källman, O., Lis, D.O., Pomorska-Wesołowska, M., Saule, M., Wisell, K.T., Vuopio, J., & Palagin, I. (2019). Antimicrobial resistance of Escherichia coli isolates from outpatient urinary tract infections in women in six European countries including Russia. Journal of Global Antimicrobial Resistance, 17, 25–34. Doi: 10.1016/J.JGAR.2018.11.004
143 Medsafe (2018). Classification of Trimethoprim Information paper for the Medicines Classification Committee. Retrieved 08/06/2022 from: https://www.medsafe.govt.nz/profs/class/Agendas/Agen60/5.3.1-MCC-Information-Paper-Trimethoprim.pdf
144 Institute for Integrated Economic Research Australia (2020). Australia’s Medical Supply Chain. Retrieved 24/08/2022 from: https://defense.info/highlight-of-the-week/australias-medical-supply-chain-addressing-strategic-vulnerabilities/
145 Rex, J.H., & Outterson, K. (2016). Antibiotic reimbursement in a model delinked from sales: A benchmark-based worldwide approach. The Lancet Infectious Diseases, 16(4), 500–505. Doi: 10.1016/S1473-3099(15)00500-9
146 Public Health Association Australia (2022, May 13). There’s more to health than hospital beds: Australia needs a Centre for Disease Control and Prevention. Retrieved 24/08/2022 from: https://www.phaa.net.au/sb_cache/associationnews/id/36/f/2022%2005%2013%20-%20There’s%20more%20to%20health%20than%20hospital%20beds%20-%20Australia%20needs%20a%20CDC%20-%20FINAL.pdf
147 Australian Healthcare and Hospitals Association (2022). An Australian Centre for Disease Control. Retrieved 2/08/2022 from: https://ahha.asn.au/sites/default/files/docs/policy-issue/australian_centre_for_disease_control_position_statement_final_1.pdf
148 Australian Medical Association (2022). AMA Submission to the Independent review of Australia’s COVID-19 response. Retrieved 24/08/2022 from: https://www.ama.com.au/articles/ama-submission-independent-review-australias-covid-19-response
149 Public Health Association Australia (2013). Towards a Framework for Communicable DIsease Control. Retrieved 24/08/2022 from: https://www.phaa.net.au/documents/item/405
150 National Centre for Antimicrobial Stewardship (2020). The National Antimicrobial Prescribing Survey. Retrieved 25/08/2022 from: https://www.ncas-australia.org/naps
151 Australian Government Department of Health and Aged Care (2022). Biotechnology in Australia – Strategic Plan for Health and Medicine. Retrieved 24/08/2022 from: https://www.health.gov.au/resources/publications/biotechnology-in-australia-strategic-plan-for-health-and-medicine